

45,000+ students realised their study abroad dream with us. Take the first step today
Meet top uk universities from the comfort of your home, here’s your new year gift, one app for all your, study abroad needs, start your journey, track your progress, grow with the community and so much more.

Verification Code
An OTP has been sent to your registered mobile no. Please verify

Thanks for your comment !
Our team will review it before it's shown to our readers.
- School Education /
Essay On Covid-19: 100, 200 and 300 Words

- Updated on
- Apr 30, 2024

COVID-19, also known as the Coronavirus, is a global pandemic that has affected people all around the world. It first emerged in a lab in Wuhan, China, in late 2019 and quickly spread to countries around the world. This virus was reportedly caused by SARS-CoV-2. Since then, it has spread rapidly to many countries, causing widespread illness and impacting our lives in numerous ways. This blog talks about the details of this virus and also drafts an essay on COVID-19 in 100, 200 and 300 words for students and professionals.
Table of Contents
- 1 Essay On COVID-19 in English 100 Words
- 2 Essay On COVID-19 in 200 Words
- 3 Essay On COVID-19 in 300 Words
- 4 Short Essay on Covid-19
Essay On COVID-19 in English 100 Words
COVID-19, also known as the coronavirus, is a global pandemic. It started in late 2019 and has affected people all around the world. The virus spreads very quickly through someone’s sneeze and respiratory issues.
COVID-19 has had a significant impact on our lives, with lockdowns, travel restrictions, and changes in daily routines. To prevent the spread of COVID-19, we should wear masks, practice social distancing, and wash our hands frequently.
People should follow social distancing and other safety guidelines and also learn the tricks to be safe stay healthy and work the whole challenging time.
Also Read: National Safe Motherhood Day 2023
Essay On COVID-19 in 200 Words
COVID-19 also known as coronavirus, became a global health crisis in early 2020 and impacted mankind around the world. This virus is said to have originated in Wuhan, China in late 2019. It belongs to the coronavirus family and causes flu-like symptoms. It impacted the healthcare systems, economies and the daily lives of people all over the world.
The most crucial aspect of COVID-19 is its highly spreadable nature. It is a communicable disease that spreads through various means such as coughs from infected persons, sneezes and communication. Due to its easy transmission leading to its outbreaks, there were many measures taken by the government from all over the world such as Lockdowns, Social Distancing, and wearing masks.
There are many changes throughout the economic systems, and also in daily routines. Other measures such as schools opting for Online schooling, Remote work options available and restrictions on travel throughout the country and internationally. Subsequently, to cure and top its outbreak, the government started its vaccine campaigns, and other preventive measures.
In conclusion, COVID-19 tested the patience and resilience of the mankind. This pandemic has taught people the importance of patience, effort and humbleness.
Also Read : Essay on My Best Friend
Essay On COVID-19 in 300 Words
COVID-19, also known as the coronavirus, is a serious and contagious disease that has affected people worldwide. It was first discovered in late 2019 in Cina and then got spread in the whole world. It had a major impact on people’s life, their school, work and daily lives.
COVID-19 is primarily transmitted from person to person through respiratory droplets produced and through sneezes, and coughs of an infected person. It can spread to thousands of people because of its highly contagious nature. To cure the widespread of this virus, there are thousands of steps taken by the people and the government.
Wearing masks is one of the essential precautions to prevent the virus from spreading. Social distancing is another vital practice, which involves maintaining a safe distance from others to minimize close contact.
Very frequent handwashing is also very important to stop the spread of this virus. Proper hand hygiene can help remove any potential virus particles from our hands, reducing the risk of infection.
In conclusion, the Coronavirus has changed people’s perspective on living. It has also changed people’s way of interacting and how to live. To deal with this virus, it is very important to follow the important guidelines such as masks, social distancing and techniques to wash your hands. Getting vaccinated is also very important to go back to normal life and cure this virus completely.
Also Read: Essay on Abortion in English in 650 Words
Short Essay on Covid-19
Please find below a sample of a short essay on Covid-19 for school students:
Also Read: Essay on Women’s Day in 200 and 500 words
to write an essay on COVID-19, understand your word limit and make sure to cover all the stages and symptoms of this disease. You need to highlight all the challenges and impacts of COVID-19. Do not forget to conclude your essay with positive precautionary measures.
Writing an essay on COVID-19 in 200 words requires you to cover all the challenges, impacts and precautions of this disease. You don’t need to describe all of these factors in brief, but make sure to add as many options as your word limit allows.
The full form for COVID-19 is Corona Virus Disease of 2019.
Related Reads
Hence, we hope that this blog has assisted you in comprehending with an essay on COVID-19. For more information on such interesting topics, visit our essay writing page and follow Leverage Edu.

Simran Popli
An avid writer and a creative person. With an experience of 1.5 years content writing, Simran has worked with different areas. From medical to working in a marketing agency with different clients to Ed-tech company, the journey has been diverse. Creative, vivacious and patient are the words that describe her personality.
Leave a Reply Cancel reply
Save my name, email, and website in this browser for the next time I comment.
Contact no. *

Connect With Us
45,000+ students realised their study abroad dream with us. take the first step today..

Resend OTP in
Need help with?
Study abroad.
UK, Canada, US & More
IELTS, GRE, GMAT & More
Scholarship, Loans & Forex
Country Preference
New Zealand
Which English test are you planning to take?
Which academic test are you planning to take.
Not Sure yet
When are you planning to take the exam?
Already booked my exam slot
Within 2 Months
Want to learn about the test
Which Degree do you wish to pursue?
When do you want to start studying abroad.
January 2024
September 2024
What is your budget to study abroad?

How would you describe this article ?
Please rate this article
We would like to hear more.
Have something on your mind?

Make your study abroad dream a reality in January 2022 with
India's Biggest Virtual University Fair

Essex Direct Admission Day
Why attend .

Don't Miss Out

Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
Introduction
The global outbreak of COVID-19 has certainly taken an overwhelming toll on everyone. People have lost their jobs, their homes, and even their lives. There is no getting past the fact that the overall impact on the world has been negative, but it is important to realize that positive aspects of the pandemic have been overshadowed by the many negative ones. In an attempt to slow the spread of the disease, many governments made the decision to implement lockdowns, forcing billions to work and take classes from home, in many cases for the first times in their lives. Not only have these lockdowns altered the way that people work and go to school, but they have altered the mental health of everyone and the environmental health of the world around us.
Connection to STS Theory
The positive impacts of technology during the pandemic stems from the Modernization Theory, posing that there is a relationship between societal and technological advancements as societies shift to become updated as opposed to traditional. Technology has brought about lots of resistance to COVID that would not have been possible without the drastic advancements in science over the years. Thanks to these advancements, relationships can stay connected, students can continue to learn, jobs can stay open, and the environment can subtly improve. Our modernized world is well enough suited to take on the troubling times that COVID-19 has brought along.
Technology with School – Relates to College Students
Remote learning has allowed each of us to learn from the comfort of our homes. Working remotely has also allowed us to work from our living rooms. The perks of both are not having to wake up early to drive to work in the mornings, not having to sit at an office desk for eight hours a day, and not having to walk to class. Working remotely and remote learning has also been a time saver for many individuals.
According to Business Insider, there are a few tips that will help students be successful while being virtual. One tip is to clean your workspace. It is important to have a space, just like you would at a desk in a classroom, to ensure that you are paying attention to the professor. It is always important to engage with your professor. It is important to contact your professor outside of the class section to ensure that you are retaining the information. Another tip that the Business Insider recommends is to connect with your classmates. It is vital to build connections with your classmates that will help everyone have a comfortable environment to ask questions.
Personal Growth
In March 2020, the COVID-19 outbreak hit the United States. College students were forced to leave their beloved campuses and go home to finish their semesters online. For some, it meant their schoolwork load was lightened and they could sleep until noon. For others, it meant their plans of graduating and having a job for the summer were in jeopardy. Regardless of their situation, one thing was likely the same for all: lots of time alone. Students found things to do to pass the time. Some learned to cook, some started exercising at home, and others had more time to do what they already loved.
Ethan, a student at the University of South Carolina, used the time to start lifting weights in his home gym. In the United States, sales of home gym equipment doubled, reaching nearly $2.4 Billion in revenue. Store shelves were entirely sold out of exercise equipment. Many students like Ethan report that exercising was one of the biggest changes they made during COVID lockdown.
Other students, such as Cam, found an opportunity to get in a better place mentally. “I learned not to take things for granted. My relationship with my family has gotten better. I’m a much stronger person,” the Clemson student reported. Grayson, an athlete at Winthrop University, reported that it made him have a more positive outlook on being by himself. A student that elected to remain anonymous was just happy they could wake up later and not have to brush their teeth as much because of masks. Whether a dentist would approve of that habit or not, an improvement in mental health is a win in anyone’s book.
A select few students decided to challenge themselves in a world where all odds are stacked against them. Dean, a freshman at the University of South Carolina, decided to start his own bracelet and T-Shirt business in a time when small businesses all over the country were facing a grave threat of going out of business. All the while, he learned to play the guitar and uploaded his songs to SoundCloud, he reported.
Whether college students decided to get a six-pack or learned how to sew, almost everyone found something constructive and positive to do with their extra free time. The college students of COVID-19 learned what it meant to make the best of an unfortunate situation. Things may have looked bleak and frightening, but they learned how to manage those feelings and make something positive out of it.
Change in Workforce
Before the pandemic, many companies did not allow employees to work from home. Also, many companies would not even allow employees to take home items, such as laptops, as a safety precaution. According to Stanford Medicine, rapid innovation and implementation of technology has allowed for the employees to navigate the challenges. It states that it is clear that technology has transformed our typical daily workflow. Technology has also made it easier to connect with the patients during the pandemic.
The Pew Research Center states “about half of new teleworkers say they have more flexibility now and that majority who are working in person worry about virus exposure.” In December 2020, 71% of the workers that were surveyed were doing their job from home all or most of the time. Of those workers, more than half said if they were given the choice that they would want to keep working from home even after the pandemic. Among those who are currently working from home, most say that it has been easy to meet deadlines and complete projects on time without interruptions.
Environmental Improvements
Before the COVID-19 outbreak, a typical day consisted of billions of people across the globe commuting to work or school, whether that be through public buses or trains, driving themselves in cars, or some other means of transportation. As all these vehicles were used, immeasurable amounts of gases and chemicals were released into the atmosphere. As infection numbers and the death toll increased, most nations began enforcing lockdown protocols, and these mandates affected almost 3 billion people (Rume & Islam, 2020). Businesses and factories shut down or people began working from home, meaning they no longer needed to drive to work. In an attempt to stunt transmission, the majority of international travel was halted, limiting tourism, which also had a great impact. Since industrialization has advanced in major cities across the globe, the amount of Greenhouse Gases that have been emitted is alarming. Cars, buses, trains, industries, factories all release harmful chemicals due to the burning of fossil fuels or other energy sources. When these pollutants enter the atmosphere, they cause a variety of issues. It decreases overall air quality and visibility, and can be dangerous to those inhali ng the m.
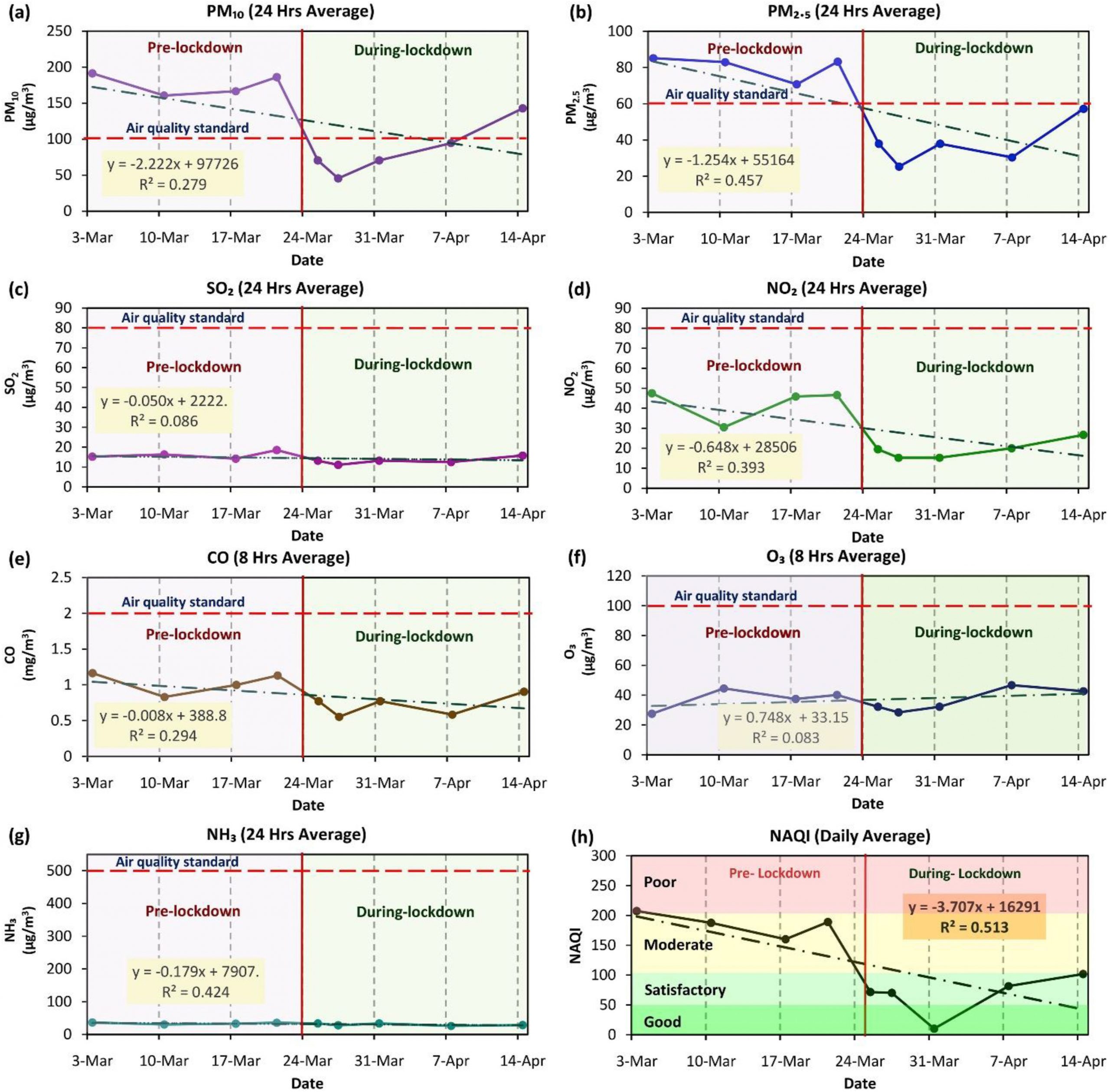
According to research performed by Shakeel Ahmad Bhat and a group of other scientists from India, China, and the United Kingdom, Delhi, India is one of the most polluted cities in the world (Bhat et al, 2021). The city is highly industrialized and densely populated, contributing to the elevated levels of particulate matter in the air. Particulate matter is small pollutant liquid droplets and solid particles in the air (Environmental Protection Agency, 2020). When inhaled, they can burrow deep into the lungs and even the bloodstream and cause serious damage to a person, “particularly respiratory ailments” (Bhat et al, 2021). The two types of particulate matter are PM10 and PM2.5, and their numbers correspond to the size of the particles (their diameters in units of micrometers). The smaller the particle, the more harmful they are. By National Ambient Air Quality Standards (NAAQS), the level of particulate matter in Delhi is well above the tolerable limits. In 2016 alone, the amount of deaths caused by the poor air quality in India “was approximately 4.2 million” (Bhat et al, 2021).
Lockdowns positively affe cted more than just the air quality around the world; additionally, water quality and beaches were a major beneficiary. Tourism for centuries has led to a significant overuse of beach resources such as fishing and leisure activities, and these in turn led to pollution of the water. If people are using jet skis and boating in lakes or oceans, the fuel and exhaust often leak into the water which can cause significant harm to the wildlife that lives in it. Restricting beach access has allowed them to recover and regain their resources, and has also decreased the pollution levels in the water. The water flowing in the Venice canals are cleaner now than they have been before (Bhat et al, 2021). pH levels, electric conductivity, dissolved oxygen levels, biochemical oxygen demand, and chemical oxygen demand have all decreased as a result of the lockdowns (Rume & Islam, 2020). These decreases all contribute to the fact that overall water quality levels have increased.
Noise pollution is an often-overlooked type of pollution that affects the world, especially in highly urbanized regions. Noise pollution is elevated levels of sound which are typically caused by human activities including transportation, machines, factories, etc. When the noise levels are elevated for extended periods of time, it negatively affects all organisms in the area. It leads to hearing loss, lack of concentration, high stress levels, interrupted sleep, and many other issues in humans. As for the wildlife, their abilities to detect and avoid predators and prey are hindered by noise pollution. It affects the invertebrates responsible for the control of many environmental processes that maintain balance in the ecosystem (Rume & Islam, 2020). When lockdowns were implemented, traveling and transportation stopped, industries shut down, flights were canceled, and people stayed home. The environment was able to recover and the people and organisms within the ecosystem enjoy a higher quality of life as a result.
Reflection Questions
- What kinds of positive experiences have you had during the pandemic?
- As stated in the chapter, there are many students who spent their time working out or picked up new hobbies. What new things were you able to focus on during the lockdowns?
Bhat, Shakeel Ahmad et al. “Impact of COVID-Related Lockdowns on Environmental and Climate Change Scenarios.” Environmental research 195 (2021): 110839–110839. Web. https://www-sciencedirect-com.libproxy.clemson.edu/science/article/pii/S001393512100133X?via%3Dihub.
DiDonato, S., Forgo, E., & Manella, H. (2020, June 5). Here’s how technology is helping residents during the COVID-19 pandemic . Scope Blog. https://scopeblog.stanford.edu/2020/06/04/how-technology-is-helping-residents-during-the-covid-19-pandemic/.
Environmental Protection Agency. (2020, October 1). Particulate Matter (PM) Basics. EPA. https://www.epa.gov/pm-pollution/particulate-matter-pm-basics.
Merkle, Steffen. “Positive Experiences During COVID-19.” Survey. 18 April 2021.
Parker, K., Horowitz, J. M., & Minkin, R. (2021, February 9). How Coronavirus Has Changed the Way Americans Work . Pew Research Center’s Social & Demographic Trends Project. https://www.pewresearch.org/social-trends/2020/12/09/how-the-coronavirus-outbreak-has-and-hasnt-changed-the-way-americans-work/.
Rume, T., & Islam, S. M. D.-U. (2020, September 17). Environmental effects of COVID-19 pandemic and potential strategies of sustainability. Heliyon. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7498239/#bib42.
Shaban, Hamza. “The Pandemic’s Home-Workout Revolution May Be Here to Stay.” The Washington Post, WP Company, 8 Jan. 2021, www.washingtonpost.com/road-to-recovery/2021/01/07/home-fitness-boom/.
Thompson, K. L. (2021, February 2). I’m a college professor who’s teaching virtually during the pandemic. Here are 7 things my most successful students do on Zoom. Business Insider. https://www.businessinsider.com/tips-for-zoom-success-as-remote-student-professor-advice-2021-2.
To the extent possible under law, Yang Wu; Allie Messenger; Arnaut Aguilar; Ashley Bui; Ava Kramer; Ben Jablonski; Blake Busking; Blake Moore; Carrie Pohlman; Brenna Turpin; Brooke Baker; Caroline Edwards; Chris Leroux; Claudia Sisk; Clayton Trentham; Davey Crouch; Eli Packer; Elle Wagner; Eliza Nix; Ellie Vensel; Erin Kennedy; Emily Cleveland; Ethan May; Ethan Hirsch; Frances Laughlin; George Easter; Grace Arnold; Grace D'Egidio; Grace Towe; Hope Wilde; Jack Sanford; Jake Brazinski; Jason McNult; Jason Saadeh; John Fuller; John Griffen; Julia Wood; Kasey Kiser; Katie Herbolsheimer; Katrina Campos; Kerrigan Donnelly; Kierstyn Stevens; Laurence Innes; Luke Dotson; Macey Coulter; Marco Guareschi; Meg Botts; Michael Havasy; Mikel Zoeller; Mitchell Wallin; Patrick Reed; Reagan Beach; Ryan Cook; Ryan Kennedy; Spencer Dalley; Steffen Merkle; Tayler Smith; Thomas Williams; Tim Egan; Tres Key; Tyler Parker; Virginia Lundeen; Will Gosnell; William Carroll; and Zoe Sabbert have waived all copyright and related or neighboring rights to COVID 19: A Student Perspective , except where otherwise noted.
Share This Book
Writing about COVID-19 in a college admission essay
by: Venkates Swaminathan | Updated: September 14, 2020
Print article

For students applying to college using the CommonApp, there are several different places where students and counselors can address the pandemic’s impact. The different sections have differing goals. You must understand how to use each section for its appropriate use.
The CommonApp COVID-19 question
First, the CommonApp this year has an additional question specifically about COVID-19 :
Community disruptions such as COVID-19 and natural disasters can have deep and long-lasting impacts. If you need it, this space is yours to describe those impacts. Colleges care about the effects on your health and well-being, safety, family circumstances, future plans, and education, including access to reliable technology and quiet study spaces. Please use this space to describe how these events have impacted you.
This question seeks to understand the adversity that students may have had to face due to the pandemic, the move to online education, or the shelter-in-place rules. You don’t have to answer this question if the impact on you wasn’t particularly severe. Some examples of things students should discuss include:
- The student or a family member had COVID-19 or suffered other illnesses due to confinement during the pandemic.
- The candidate had to deal with personal or family issues, such as abusive living situations or other safety concerns
- The student suffered from a lack of internet access and other online learning challenges.
- Students who dealt with problems registering for or taking standardized tests and AP exams.
Jeff Schiffman of the Tulane University admissions office has a blog about this section. He recommends students ask themselves several questions as they go about answering this section:
- Are my experiences different from others’?
- Are there noticeable changes on my transcript?
- Am I aware of my privilege?
- Am I specific? Am I explaining rather than complaining?
- Is this information being included elsewhere on my application?
If you do answer this section, be brief and to-the-point.
Counselor recommendations and school profiles
Second, counselors will, in their counselor forms and school profiles on the CommonApp, address how the school handled the pandemic and how it might have affected students, specifically as it relates to:
- Grading scales and policies
- Graduation requirements
- Instructional methods
- Schedules and course offerings
- Testing requirements
- Your academic calendar
- Other extenuating circumstances
Students don’t have to mention these matters in their application unless something unusual happened.
Writing about COVID-19 in your main essay
Write about your experiences during the pandemic in your main college essay if your experience is personal, relevant, and the most important thing to discuss in your college admission essay. That you had to stay home and study online isn’t sufficient, as millions of other students faced the same situation. But sometimes, it can be appropriate and helpful to write about something related to the pandemic in your essay. For example:
- One student developed a website for a local comic book store. The store might not have survived without the ability for people to order comic books online. The student had a long-standing relationship with the store, and it was an institution that created a community for students who otherwise felt left out.
- One student started a YouTube channel to help other students with academic subjects he was very familiar with and began tutoring others.
- Some students used their extra time that was the result of the stay-at-home orders to take online courses pursuing topics they are genuinely interested in or developing new interests, like a foreign language or music.
Experiences like this can be good topics for the CommonApp essay as long as they reflect something genuinely important about the student. For many students whose lives have been shaped by this pandemic, it can be a critical part of their college application.
Want more? Read 6 ways to improve a college essay , What the &%$! should I write about in my college essay , and Just how important is a college admissions essay? .
Homes Nearby
Homes for rent and sale near schools

How our schools are (and aren't) addressing race

The truth about homework in America

What should I write my college essay about?
What the #%@!& should I write about in my college essay?
Yes! Sign me up for updates relevant to my child's grade.
Please enter a valid email address
Thank you for signing up!
Server Issue: Please try again later. Sorry for the inconvenience
- Today's news
- Reviews and deals
- Climate change
- 2024 election
- Newsletters
- Fall allergies
- Health news
- Mental health
- Sexual health
- Family health
- So mini ways
- Unapologetically
- Buying guides
Entertainment
- How to Watch
- My watchlist
- Stock market
- Biden economy
- Personal finance
- Stocks: most active
- Stocks: gainers
- Stocks: losers
- Trending tickers
- World indices
- US Treasury bonds
- Top mutual funds
- Highest open interest
- Highest implied volatility
- Currency converter
- Basic materials
- Communication services
- Consumer cyclical
- Consumer defensive
- Financial services
- Industrials
- Real estate
- Mutual funds
- Credit cards
- Balance transfer cards
- Cash back cards
- Rewards cards
- Travel cards
- Online checking
- High-yield savings
- Money market
- Home equity loan
- Personal loans
- Student loans
- Options pit
- Fantasy football
- Pro Pick 'Em
- College Pick 'Em
- Fantasy baseball
- Fantasy hockey
- Fantasy basketball
- Download the app
- Daily fantasy
- Scores and schedules
- GameChannel
- World Baseball Classic
- Premier League
- CONCACAF League
- Champions League
- Motorsports
- Horse racing
New on Yahoo
- Privacy Dashboard
How to Write About the Impact of the Coronavirus in a College Essay
The global impact of COVID-19, the disease caused by the novel coronavirus, means colleges and prospective students alike are in for an admissions cycle like no other. Both face unprecedented challenges and questions as they grapple with their respective futures amid the ongoing fallout of the pandemic.
Colleges must examine applicants without the aid of standardized test scores for many -- a factor that prompted many schools to go test-optional for now . Even grades, a significant component of a college application, may be hard to interpret with some high schools adopting pass-fail classes last spring due to the pandemic. Major college admissions factors are suddenly skewed.
"I can't help but think other (admissions) factors are going to matter more," says Ethan Sawyer, founder of the College Essay Guy, a website that offers free and paid essay-writing resources.
College essays and letters of recommendation , Sawyer says, are likely to carry more weight than ever in this admissions cycle. And many essays will likely focus on how the pandemic shaped students' lives throughout an often tumultuous 2020.
[ Read: How to Write a College Essay. ]
But before writing a college essay focused on the coronavirus, students should explore whether it's the best topic for them.
Writing About COVID-19 for a College Application
Much of daily life has been colored by the coronavirus. Virtual learning is the norm at many colleges and high schools, many extracurriculars have vanished and social lives have stalled for students complying with measures to stop the spread of COVID-19.
"For some young people, the pandemic took away what they envisioned as their senior year," says Robert Alexander, dean of admissions, financial aid and enrollment management at the University of Rochester in New York. "Maybe that's a spot on a varsity athletic team or the lead role in the fall play. And it's OK for them to mourn what should have been and what they feel like they lost, but more important is how are they making the most of the opportunities they do have?"
That question, Alexander says, is what colleges want answered if students choose to address COVID-19 in their college essay.
But the question of whether a student should write about the coronavirus is tricky. The answer depends largely on the student.
"In general, I don't think students should write about COVID-19 in their main personal statement for their application," Robin Miller, master college admissions counselor at IvyWise, a college counseling company, wrote in an email.
"Certainly, there may be exceptions to this based on a student's individual experience, but since the personal essay is the main place in the application where the student can really allow their voice to be heard and share insight into who they are as an individual, there are likely many other topics they can choose to write about that are more distinctive and unique than COVID-19," Miller says.
[ Read: What Colleges Look for: 6 Ways to Stand Out. ]
Opinions among admissions experts vary on whether to write about the likely popular topic of the pandemic.
"If your essay communicates something positive, unique, and compelling about you in an interesting and eloquent way, go for it," Carolyn Pippen, principal college admissions counselor at IvyWise, wrote in an email. She adds that students shouldn't be dissuaded from writing about a topic merely because it's common, noting that "topics are bound to repeat, no matter how hard we try to avoid it."
Above all, she urges honesty.
"If your experience within the context of the pandemic has been truly unique, then write about that experience, and the standing out will take care of itself," Pippen says. "If your experience has been generally the same as most other students in your context, then trying to find a unique angle can easily cross the line into exploiting a tragedy, or at least appearing as though you have."
But focusing entirely on the pandemic can limit a student to a single story and narrow who they are in an application, Sawyer says. "There are so many wonderful possibilities for what you can say about yourself outside of your experience within the pandemic."
He notes that passions, strengths, career interests and personal identity are among the multitude of essay topic options available to applicants and encourages them to probe their values to help determine the topic that matters most to them -- and write about it.
That doesn't mean the pandemic experience has to be ignored if applicants feel the need to write about it.
Writing About Coronavirus in Main and Supplemental Essays
Students can choose to write a full-length college essay on the coronavirus or summarize their experience in a shorter form.
To help students explain how the pandemic affected them, The Common App has added an optional section to address this topic. Applicants have 250 words to describe their pandemic experience and the personal and academic impact of COVID-19.
[ Read: The Common App: Everything You Need to Know. ]
"That's not a trick question, and there's no right or wrong answer," Alexander says. Colleges want to know, he adds, how students navigated the pandemic, how they prioritized their time, what responsibilities they took on and what they learned along the way.
If students can distill all of the above information into 250 words, there's likely no need to write about it in a full-length college essay, experts say. And applicants whose lives were not heavily altered by the pandemic may even choose to skip the optional COVID-19 question.
"This space is best used to discuss hardship and/or significant challenges that the student and/or the student's family experienced as a result of COVID-19 and how they have responded to those difficulties," Miller notes. Using the section to acknowledge a lack of impact, she adds, "could be perceived as trite and lacking insight, despite the good intentions of the applicant."
To guard against this lack of awareness, Sawyer encourages students to tap someone they trust to review their writing , whether it's the 250-word Common App response or the full-length essay.
Experts tend to agree that the short-form approach to this as an essay topic works better, but there are exceptions. And if a student does have a coronavirus story that he or she feels must be told, Alexander encourages the writer to be authentic in the essay.
"My advice for an essay about COVID-19 is the same as my advice about an essay for any topic -- and that is, don't write what you think we want to read or hear," Alexander says. "Write what really changed you and that story that now is yours and yours alone to tell."
Sawyer urges students to ask themselves, "What's the sentence that only I can write?" He also encourages students to remember that the pandemic is only a chapter of their lives and not the whole book.
Miller, who cautions against writing a full-length essay on the coronavirus, says that if students choose to do so they should have a conversation with their high school counselor about whether that's the right move. And if students choose to proceed with COVID-19 as a topic, she says they need to be clear, detailed and insightful about what they learned and how they adapted along the way.
"Approaching the essay in this manner will provide important balance while demonstrating personal growth and vulnerability," Miller says.
Pippen encourages students to remember that they are in an unprecedented time for college admissions.
"It is important to keep in mind with all of these (admission) factors that no colleges have ever had to consider them this way in the selection process, if at all," Pippen says. "They have had very little time to calibrate their evaluations of different application components within their offices, let alone across institutions. This means that colleges will all be handling the admissions process a little bit differently, and their approaches may even evolve over the course of the admissions cycle."
Searching for a college? Get our complete rankings of Best Colleges.
- Share full article
Advertisement
Supported by
‘When Normal Life Stopped’: College Essays Reflect a Turbulent Year
This year’s admissions essays became a platform for high school seniors to reflect on the pandemic, race and loss.

By Anemona Hartocollis
This year perhaps more than ever before, the college essay has served as a canvas for high school seniors to reflect on a turbulent and, for many, sorrowful year. It has been a psychiatrist’s couch, a road map to a more hopeful future, a chance to pour out intimate feelings about loneliness and injustice.
In response to a request from The New York Times, more than 900 seniors submitted the personal essays they wrote for their college applications. Reading them is like a trip through two of the biggest news events of recent decades: the devastation wrought by the coronavirus, and the rise of a new civil rights movement.
In the wake of the high-profile deaths of Black people like George Floyd and Breonna Taylor at the hands of police officers, students shared how they had wrestled with racism in their own lives. Many dipped their feet into the politics of protest, finding themselves strengthened by their activism, yet sometimes conflicted.
And in the midst of the most far-reaching pandemic in a century, they described the isolation and loss that have pervaded every aspect of their lives since schools suddenly shut down a year ago. They sought to articulate how they have managed while cut off from friends and activities they had cultivated for years.
To some degree, the students were responding to prompts on the applications, with their essays taking on even more weight in a year when many colleges waived standardized test scores and when extracurricular activities were wiped out.
We are having trouble retrieving the article content.
Please enable JavaScript in your browser settings.
Thank you for your patience while we verify access. If you are in Reader mode please exit and log into your Times account, or subscribe for all of The Times.
Thank you for your patience while we verify access.
Already a subscriber? Log in .
Want all of The Times? Subscribe .
What Life Was Like for Students in the Pandemic Year

- Share article
In this video, Navajo student Miles Johnson shares how he experienced the stress and anxiety of schools shutting down last year. Miles’ teacher shared his experience and those of her other students in a recent piece for Education Week. In these short essays below, teacher Claire Marie Grogan’s 11th grade students at Oceanside High School on Long Island, N.Y., describe their pandemic experiences. Their writings have been slightly edited for clarity. Read Grogan’s essay .
“Hours Staring at Tiny Boxes on the Screen”
By Kimberly Polacco, 16
I stare at my blank computer screen, trying to find the motivation to turn it on, but my finger flinches every time it hovers near the button. I instead open my curtains. It is raining outside, but it does not matter, I will not be going out there for the rest of the day. The sound of pounding raindrops contributes to my headache enough to make me turn on my computer in hopes that it will give me something to drown out the noise. But as soon as I open it up, I feel the weight of the world crash upon my shoulders.
Each 42-minute period drags on by. I spend hours upon hours staring at tiny boxes on a screen, one of which my exhausted face occupies, and attempt to retain concepts that have been presented to me through this device. By the time I have the freedom of pressing the “leave” button on my last Google Meet of the day, my eyes are heavy and my legs feel like mush from having not left my bed since I woke up.
Tomorrow arrives, except this time here I am inside of a school building, interacting with my first period teacher face to face. We talk about our favorite movies and TV shows to stream as other kids pile into the classroom. With each passing period I accumulate more and more of these tiny meaningless conversations everywhere I go with both teachers and students. They may not seem like much, but to me they are everything because I know that the next time I am expected to report to school, I will be trapped in the bubble of my room counting down the hours until I can sit down in my freshly sanitized wooden desk again.
“My Only Parent Essentially on Her Death Bed”
By Nick Ingargiola, 16
My mom had COVID-19 for ten weeks. She got sick during the first month school buildings were shut. The difficulty of navigating an online classroom was already overwhelming, and when mixed with my only parent essentially on her death bed, it made it unbearable. Focusing on schoolwork was impossible, and watching my mother struggle to lift up her arm broke my heart.
My mom has been through her fair share of diseases from pancreatic cancer to seizures and even as far as a stroke that paralyzed her entire left side. It is safe to say she has been through a lot. The craziest part is you would never know it. She is the strongest and most positive person I’ve ever met. COVID hit her hard. Although I have watched her go through life and death multiple times, I have never seen her so physically and mentally drained.
I initially was overjoyed to complete my school year in the comfort of my own home, but once my mom got sick, I couldn’t handle it. No one knows what it’s like to pretend like everything is OK until they are forced to. I would wake up at 8 after staying up until 5 in the morning pondering the possibility of losing my mother. She was all I had. I was forced to turn my camera on and float in the fake reality of being fine although I wasn’t. The teachers tried to keep the class engaged by obligating the students to participate. This was dreadful. I didn’t want to talk. I had to hide the distress in my voice. If only the teachers understood what I was going through. I was hesitant because I didn’t want everyone to know that the virus that was infecting and killing millions was knocking on my front door.
After my online classes, I was required to finish an immense amount of homework while simultaneously hiding my sadness so that my mom wouldn’t worry about me. She was already going through a lot. There was no reason to add me to her list of worries. I wasn’t even able to give her a hug. All I could do was watch.
“The Way of Staying Sane”
By Lynda Feustel, 16
Entering year two of the pandemic is strange. It barely seems a day since last March, but it also seems like a lifetime. As an only child and introvert, shutting down my world was initially simple and relatively easy. My friends and I had been super busy with the school play, and while I was sad about it being canceled, I was struggling a lot during that show and desperately needed some time off.
As March turned to April, virtual school began, and being alone really set in. I missed my friends and us being together. The isolation felt real with just my parents and me, even as we spent time together. My friends and I began meeting on Facetime every night to watch TV and just be together in some way. We laughed at insane jokes we made and had homework and therapy sessions over Facetime and grew closer through digital and literal walls.
The summer passed with in-person events together, and the virus faded into the background for a little while. We went to the track and the beach and hung out in people’s backyards.
Then school came for us in a more nasty way than usual. In hybrid school we were separated. People had jobs, sports, activities, and quarantines. Teachers piled on work, and the virus grew more present again. The group text put out hundreds of messages a day while the Facetimes came to a grinding halt, and meeting in person as a group became more of a rarity. Being together on video and in person was the way of staying sane.
In a way I am in a similar place to last year, working and looking for some change as we enter the second year of this mess.
“In History Class, Reports of Heightening Cases”
By Vivian Rose, 16
I remember the moment my freshman year English teacher told me about the young writers’ conference at Bread Loaf during my sophomore year. At first, I didn’t want to apply, the deadline had passed, but for some strange reason, the directors of the program extended it another week. It felt like it was meant to be. It was in Vermont in the last week of May when the flowers have awakened and the sun is warm.
I submitted my work, and two weeks later I got an email of my acceptance. I screamed at the top of my lungs in the empty house; everyone was out, so I was left alone to celebrate my small victory. It was rare for them to admit sophomores. Usually they accept submissions only from juniors and seniors.
That was the first week of February 2020. All of a sudden, there was some talk about this strange virus coming from China. We thought nothing of it. Every night, I would fall asleep smiling, knowing that I would be able to go to the exact conference that Robert Frost attended for 42 years.
Then, as if overnight, it seemed the virus had swung its hand and had gripped parts of the country. Every newscast was about the disease. Every day in history, we would look at the reports of heightening cases and joke around that this could never become a threat as big as Dr. Fauci was proposing. Then, March 13th came around--it was the last day before the world seemed to shut down. Just like that, Bread Loaf would vanish from my grasp.
“One Day Every Day Won’t Be As Terrible”
By Nick Wollweber, 17
COVID created personal problems for everyone, some more serious than others, but everyone had a struggle.
As the COVID lock-down took hold, the main thing weighing on my mind was my oldest brother, Joe, who passed away in January 2019 unexpectedly in his sleep. Losing my brother was a complete gut punch and reality check for me at 14 and 15 years old. 2019 was a year of struggle, darkness, sadness, frustration. I didn’t want to learn after my brother had passed, but I had to in order to move forward and find my new normal.
Routine and always having things to do and places to go is what let me cope in the year after Joe died. Then COVID came and gave me the option to let up and let down my guard. I struggled with not wanting to take care of personal hygiene. That was the beginning of an underlying mental problem where I wouldn’t do things that were necessary for everyday life.
My “coping routine” that got me through every day and week the year before was gone. COVID wasn’t beneficial to me, but it did bring out the true nature of my mental struggles and put a name to it. Since COVID, I have been diagnosed with severe depression and anxiety. I began taking antidepressants and going to therapy a lot more.
COVID made me realize that I’m not happy with who I am and that I needed to change. I’m still not happy with who I am. I struggle every day, but I am working towards a goal that one day every day won’t be as terrible.
Coverage of social and emotional learning is supported in part by a grant from the NoVo Foundation, at www.novofoundation.org . Education Week retains sole editorial control over the content of this coverage. A version of this article appeared in the March 31, 2021 edition of Education Week as What Life Was Like for Students in the Pandemic Year

Sign Up for The Savvy Principal
Edweek top school jobs.

Sign Up & Sign In

Students’ Essays on Infectious Disease Prevention, COVID-19 Published Nationwide

As part of the BIO 173: Global Change and Infectious Disease course, Professor Fred Cohan assigns students to write an essay persuading others to prevent future and mitigate present infectious diseases. If students submit their essay to a news outlet—and it’s published—Cohan awards them with extra credit.
As a result of this assignment, more than 25 students have had their work published in newspapers across the United States. Many of these essays cite and applaud the University’s Keep Wes Safe campaign and its COVID-19 testing protocols.
Cohan, professor of biology and Huffington Foundation Professor in the College of the Environment (COE), began teaching the Global Change and Infectious Disease course in 2009, when the COE was established. “I wanted very much to contribute a course to what I saw as a real game-changer in Wesleyan’s interest in the environment. The course is about all the ways that human demands on the environment have brought us infectious diseases, over past millennia and in the present, and why our environmental disturbances will continue to bring us infections into the future.”
Over the years, Cohan learned that he can sustainably teach about 170 students every year without running out of interested students. This fall, he had 207. Although he didn’t change the overall structure of his course to accommodate COVID-19 topics, he did add material on the current pandemic to various sections of the course.
“I wouldn’t say that the population of the class increased tremendously as a result of COVID-19, but I think the enthusiasm of the students for the material has increased substantially,” he said.
To accommodate online learning, Cohan shaved off 15 minutes from his normal 80-minute lectures to allow for discussion sections, led by Cohan and teaching assistants. “While the lectures mostly dealt with biology, the discussions focused on how changes in behavior and policy can solve the infectious disease problems brought by human disturbance of the environment,” he said.
Based on student responses to an introspective exam question, Cohan learned that many students enjoyed a new hope that we could each contribute to fighting infectious disease. “They discovered that the solution to infectious disease is not entirely a waiting game for the right technologies to come along,” he said. “Many enjoyed learning about fighting infectious disease from a moral and social perspective. And especially, the students enjoyed learning about the ‘socialism of the microbe,’ how preventing and curing others’ infections will prevent others’ infections from becoming our own. The students enjoyed seeing how this idea can drive both domestic and international health policies.”
A sampling of the published student essays are below:
Alexander Giummo ’22 and Mike Dunderdale’s ’23 op-ed titled “ A National Testing Proposal: Let’s Fight Back Against COVID-19 ” was published in the Journal Inquirer in Manchester, Conn.
They wrote: “With an expansive and increased testing plan for U.S. citizens, those who are COVID-positive could limit the number of contacts they have, and this would also help to enable more effective contact tracing. Testing could also allow for the return of some ‘normal’ events, such as small social gatherings, sports, and in-person class and work schedules.
“We propose a national testing strategy in line with the one that has kept Wesleyan students safe this year. The plan would require a strong push by the federal government to fund the initiative, but it is vital to successful containment of the virus.
“Twice a week, all people living in the U.S. should report to a local testing site staffed with professionals where the anterior nasal swab Polymerase Chain Reaction (PCR) test, used by Wesleyan and supported by the Broad Institute, would be implemented.”
Kalyani Mohan ’22 and Kalli Jackson ’22 penned an essay titled “ Where Public Health Meets Politics: COVID-19 in the United States ,” which was published in Wesleyan’s Arcadia Political Review .
They wrote: “While the U.S. would certainly benefit from a strengthened pandemic response team and structural changes to public health systems, that alone isn’t enough, as American society is immensely stratified, socially and culturally. The politicization of the COVID-19 pandemic shows that individualism, libertarianism and capitalism are deeply ingrained in American culture, to the extent that Americans often blind to the fact community welfare can be equivalent to personal welfare. Pandemics are multifaceted, and preventing them requires not just a cultural shift but an emotional one amongst the American people, one guided by empathy—towards other people, different communities and the planet. Politics should be a tool, not a weapon against its people.”
Sydnee Goyer ’21 and Marcel Thompson’s ’22 essay “ This Flu Season Will Be Decisive in the Fight Against COVID-19 ” also was published in Arcadia Political Review .
“With winter approaching all around the Northern Hemisphere, people are preparing for what has already been named a “twindemic,” meaning the joint threat of the coronavirus and the seasonal flu,” they wrote. “While it is known that seasonal vaccinations reduce the risk of getting the flu by up to 60% and also reduce the severity of the illness after the contamination, additional research has been conducted in order to know whether or not flu shots could reduce the risk of people getting COVID-19. In addition to the flu shot, it is essential that people remain vigilant in maintaining proper social distancing, washing your hands thoroughly, and continuing to wear masks in public spaces.”
An op-ed titled “ The Pandemic Has Shown Us How Workplace Culture Needs to Change ,” written by Adam Hickey ’22 and George Fuss ’21, was published in Park City, Utah’s The Park Record .
They wrote: “One review of academic surveys (most of which were conducted in the United States) conducted in 2019 found that between 35% and 97% of respondents in those surveys reported having attended work while they were ill, often because of workplace culture or policy which generated pressure to do so. Choosing to ignore sickness and return to the workplace while one is ill puts colleagues at risk, regardless of the perceived severity of your own illness; COVID-19 is an overbearing reminder that a disease that may cause mild, even cold-like symptoms for some can still carry fatal consequences for others.
“A mandatory paid sick leave policy for every worker, ideally across the globe, would allow essential workers to return to work when necessary while still providing enough wiggle room for economically impoverished employees to take time off without going broke if they believe they’ve contracted an illness so as not to infect the rest of their workplace and the public at large.”

Women’s cross country team members and classmates Jane Hollander ’23 and Sara Greene ’23 wrote a sports-themed essay titled “ This Season, High School Winter Sports Aren’t Worth the Risk ,” which was published in Tap into Scotch Plains/Fanwood , based in Scotch Plains, N.J. Their essay focused on the risks high school sports pose on student-athletes, their families, and the greater community.
“We don’t propose cutting off sports entirely— rather, we need to be realistic about the levels at which athletes should be participating. There are ways to make practices safer,” they wrote. “At [Wesleyan], we began the season in ‘cohorts,’ so the amount of people exposed to one another would be smaller. For non-contact sports, social distancing can be easily implemented, and for others, teams can focus on drills, strength and conditioning workouts, and skill-building exercises. Racing sports such as swim and track can compete virtually, comparing times with other schools, and team sports can focus their competition on intra-team scrimmages. These changes can allow for the continuation of a sense of normalcy and team camaraderie without the exposure to students from different geographic areas in confined, indoor spaces.”
Brook Guiffre ’23 and Maddie Clarke’s ’22 op-ed titled “ On the Pandemic ” was published in Hometown Weekly, based in Medfield, Mass.
“The first case of COVID-19 in the United States was recorded on January 20th, 2020. For the next month and a half, the U.S. continued operating normally, while many other countries began their lockdown,” they wrote. “One month later, on February 29th, 2020, the federal government approved a national testing program, but it was too little too late. The U.S. was already in pandemic mode, and completely unprepared. Frontline workers lacked access to N-95 masks, infected patients struggled to get tested, and national leaders informed the public that COVID-19 was nothing more than the common flu. Ultimately, this unpreparedness led to thousands of avoidable deaths and long-term changes to daily life. With the risk of novel infectious diseases emerging in the future being high, it is imperative that the U.S. learn from its failure and better prepare for future pandemics now. By strengthening our public health response and re-establishing government organizations specialized in disease control, we have the ability to prevent more years spent masked and six feet apart.”
In addition, their other essay, “ On Mass Extinction ,” was also published by Hometown Weekly .
“The sixth mass extinction—which scientists have coined as the Holocene Extinction—is upon us. According to the United Nations, around one million plant and animal species are currently in danger of extinction, and many more within the next decade. While other extinctions have occurred in Earth’s history, none have occurred at such a rapid rate,” they wrote. “For the sake of both biodiversity and infectious diseases, it is in our best interest to stop pushing this Holocene Extinction further.”
An essay titled “ Learning from Our Mistakes: How to Protect Ourselves and Our Communities from Diseases ,” written by Nicole Veru ’21 and Zoe Darmon ’21, was published in My Hometown Bronxville, based in Bronxville, N.Y.
“We can protect ourselves and others from future infectious diseases by ensuring that we are vaccinated,” they wrote. “Vaccines have high levels of success if enough people get them. Due to vaccines, society is no longer ravaged by childhood diseases such as mumps, rubella, measles, and smallpox. We have been able to eradicate diseases through vaccines; smallpox, one of the world’s most consequential diseases, was eradicated from the world in the 1970s.
“In 2000, the U.S. was nearly free of measles, yet, due to hesitations by anti-vaxxers, there continues to be cases. From 2000–2015 there were over 18 measles outbreaks in the U.S. This is because unless a disease is completely eradicated, there will be a new generation susceptible.
“Although vaccines are not 100% effective at preventing infection, if we continue to get vaccinated, we protect ourselves and those around us. If enough people are vaccinated, societies can develop herd immunity. The amount of people vaccinated to obtain herd immunity depends on the disease, but if this fraction is obtained, the spread of disease is contained. Through herd immunity, we protect those who may not be able to get vaccinated, such as people who are immunocompromised and the tiny portion of people for whom the vaccine is not effective.”
Dhruvi Rana ’22 and Bryce Gillis ’22 co-authored an op-ed titled “ We Must Educate Those Who Remain Skeptical of the Dangers of COVID-19 ,” which was published in Rhode Island Central .
“As Rhode Island enters the winter season, temperatures are beginning to drop and many studies have demonstrated that colder weather and lower humidity are correlated with higher transmissibility of SARS-CoV-2, the virus that causes COVID-19,” they wrote. “By simply talking or breathing, we release respiratory droplets and aerosols (tiny fluid particles which could carry the coronavirus pathogen), which can remain in the air for minutes to hours.
“In order to establish herd immunity in the US, we must educate those who remain skeptical of the dangers of COVID-19. Whether community-driven or state-funded, educational campaigns are needed to ensure that everyone fully comprehends how severe COVID-19 is and the significance of airborne transmission. While we await a vaccine, it is necessary now more than ever that we social distance, avoid crowds, and wear masks, given that colder temperatures will likely yield increased transmission of the virus.”
Danielle Rinaldi ’21 and Verónica Matos Socorro ’21 published their op-ed titled “ Community Forum: How Mask-Wearing Demands a Cultural Reset ” in the Ewing Observer , based in Lawrence, N.J.
“In their own attempt to change personal behavior during the pandemic, Wesleyan University has mandated mask-wearing in almost every facet of campus life,” they wrote. “As members of our community, we must recognize that mask-wearing is something we are all responsible and accountable for, not only because it is a form of protection for us, but just as important for others as well. However, it seems as though both Covid fatigue and complacency are dominating the mindsets of Americans, leading to even more unwillingness to mask up. Ultimately, it is inevitable that this pandemic will not be the last in our lifespan due to global warming creating irreversible losses in biodiversity. As a result, it is imperative that we adopt the norm of mask-wearing now and undergo a culture shift of the abandonment of an individualistic mindset, and instead, create a society that prioritizes taking care of others for the benefit of all.”

Shayna Dollinger ’22 and Hayley Lipson ’21 wrote an essay titled “ My Pandemic Year in College Has Brought Pride and Purpose. ” Dollinger submitted the piece, rewritten in first person, to Jewish News of Northern California . Read more about Dollinger’s publication in this News @ Wesleyan article .
“I lay in the dead grass, a 6-by-6-foot square all to myself. I cheer for my best friend, who is on the stage constructed at the bottom of Foss hill, dancing with her Bollywood dance group. Masks cover their ordinarily smiling faces as their bodies move in sync. Looking around at friends and classmates, each in their own 6-by-6 world, I feel an overwhelming sense of normalcy.
“One of the ways in which Wesleyan has prevented outbreaks on campus is by holding safe, socially distanced events that students want to attend. By giving us places to be and things to do on the weekends, we are discouraged from breaking rules and causing outbreaks at ‘super-spreader’ events.”
An op-ed written by Luna Mac-Williams ’22 and Daëlle Coriolan ’24 titled “ Collectivist Practices to Combat COVID-19 ” was published in the Wesleyan Argus .
“We are embroiled in a global pandemic that disproportionately affects poor communities of color, and in the midst of a higher cultural consciousness of systemic inequities,” they wrote. “A cultural shift to center collectivist thought and action not only would prove helpful in disease prevention, but also belongs in conversation with the Black Lives Matter movement. Collectivist models of thinking effectively target the needs of vulnerable populations including the sick, the disenfranchised, the systematically marginalized. Collectivist systems provide care, decentering the capitalist, individualist system, and focusing on how communities can work to be self-sufficient and uplift our own neighbors.”
An essay written by Maria Noto ’21 , titled “ U.S. Individualism Has Deadly Consequences ,” is published in the Oneonta Daily Star , based in Oneonta, N.Y.
She wrote, “When analyzing the cultures of certain East Asian countries, several differences stand out. For instance, when people are sick and during the cold and flu season, many East Asian cultures, including South Korea, use mask-wearing. What is considered a threat to freedom by some Americans is a preventive action and community obligation in this example. This, along with many other cultural differences, is insightful in understanding their ability to contain the virus.
“These differences are deeply seeded in the values of a culture. However, there is hope for the U.S. and other individualistic cultures in recognizing and adopting these community-centered approaches. Our mindset needs to be revolutionized with the help of federal and local assistance: mandating masks, passing another stimulus package, contact tracing, etc… However, these measures will be unsuccessful unless everyone participates for the good of a community.”

A published op-ed by Madison Szabo ’23 , Caitlyn Ferrante ’23 ran in the Two Rivers Times . The piece is titled “ Anxiety and Aspiration: Analyzing the Politicization of the Pandemic .”
John Lee ’21 and Taylor Goodman-Leong ’21 have published their op-ed titled “ Reassessing the media’s approach to COVID-19 ” in Weekly Monday Cafe 24 (Page 2).
An essay by Eleanor Raab ’21 and Elizabeth Nefferdorf ’22 titled “ Preventing the Next Epidemic ” was published in The Almanac .
- Keep Wes Safe
- student publications
- Teaching during the pandemic
Related Articles
Wesleyan in the News: September 2024
Wesleyan Fulbright Fellows Embark on Global Journeys of Curiosity
Updates on new science building, integrative arts lab construction, previous matesan's new book explores political violence, islamist mobilization in egypt and indonesia, next students launch fun, interactive virtual program for school-aged kids.
- How to Order
Persuasive Essay Guide
Persuasive Essay About Covid19
How to Write a Persuasive Essay About Covid19 | Examples & Tips
14 min read

People also read
A Comprehensive Guide to Writing an Effective Persuasive Essay
A Catalogue of 300 Best Persuasive Essay Topics for Students
Persuasive Essay Outline - A Complete Guide
30+ Persuasive Essay Examples To Get You Started
Read Excellent Examples of Persuasive Essay About Gun Control
How To Write A Persuasive Essay On Abortion
Learn to Write a Persuasive Essay About Business With 5 Best Examples
Check Out 14 Persuasive Essays About Online Education Examples
Persuasive Essay About Smoking - Making a Powerful Argument with Examples
Are you looking to write a persuasive essay about the Covid-19 pandemic?
Writing a compelling and informative essay about this global crisis can be challenging. It requires researching the latest information, understanding the facts, and presenting your argument persuasively.
But don’t worry! with some guidance from experts, you’ll be able to write an effective and persuasive essay about Covid-19.
In this blog post, we’ll outline the basics of writing a persuasive essay . We’ll provide clear examples, helpful tips, and essential information for crafting your own persuasive piece on Covid-19.
Read on to get started on your essay.
- 1. Steps to Write a Persuasive Essay About Covid-19
- 2. Examples of Persuasive Essay About COVID-19
- 3. Examples of Persuasive Essay About COVID-19 Vaccine
- 4. Examples of Persuasive Essay About COVID-19 Integration
- 5. Examples of Argumentative Essay About Covid 19
- 6. Examples of Persuasive Speeches About Covid-19
- 7. Tips to Write a Persuasive Essay About Covid-19
- 8. Common Topics for a Persuasive Essay on COVID-19
Steps to Write a Persuasive Essay About Covid-19
Here are the steps to help you write a persuasive essay on this topic, along with an example essay:
Step 1: Choose a Specific Thesis Statement
Your thesis statement should clearly state your position on a specific aspect of COVID-19. It should be debatable and clear. For example:
| "COVID-19 vaccination mandates are necessary for public health and safety." |
Step 2: Research and Gather Information
Collect reliable and up-to-date information from reputable sources to support your thesis statement. This may include statistics, expert opinions, and scientific studies. For instance:
- COVID-19 vaccination effectiveness data
- Information on vaccine mandates in different countries
- Expert statements from health organizations like the WHO or CDC
Step 3: Outline Your Essay
Create a clear and organized outline to structure your essay. A persuasive essay typically follows this structure:
- Introduction
- Background Information
- Body Paragraphs (with supporting evidence)
- Counterarguments (addressing opposing views)
Step 4: Write the Introduction
In the introduction, grab your reader's attention and present your thesis statement. For example:
| The COVID-19 pandemic has presented an unprecedented global challenge, and in the face of this crisis, many countries have debated the implementation of vaccination mandates. This essay argues that such mandates are essential for safeguarding public health and preventing further devastation caused by the virus. |
Step 5: Provide Background Information
Offer context and background information to help your readers understand the issue better. For instance:
| COVID-19, caused by the novel coronavirus SARS-CoV-2, emerged in late 2019 and quickly spread worldwide, leading to millions of infections and deaths. Vaccination has proven to be an effective tool in curbing the virus's spread and severity. |
Step 6: Develop Body Paragraphs
Each body paragraph should present a single point or piece of evidence that supports your thesis statement. Use clear topic sentences , evidence, and analysis. Here's an example:
| One compelling reason for implementing COVID-19 vaccination mandates is the overwhelming evidence of vaccine effectiveness. According to a study published in the New England Journal of Medicine, the Pfizer-BioNTech and Moderna vaccines demonstrated an efficacy of over 90% in preventing symptomatic COVID-19 cases. This level of protection not only reduces the risk of infection but also minimizes the virus's impact on healthcare systems. |
Step 7: Address Counterarguments
Acknowledge opposing viewpoints and refute them with strong counterarguments. This demonstrates that you've considered different perspectives. For example:
| Some argue that vaccination mandates infringe on personal freedoms and autonomy. While individual freedom is a crucial aspect of democratic societies, public health measures have long been implemented to protect the collective well-being. Seatbelt laws, for example, are in place to save lives, even though they restrict personal choice. |
Step 8: Write the Conclusion
Summarize your main points and restate your thesis statement in the conclusion. End with a strong call to action or thought-provoking statement. For instance:
| In conclusion, COVID-19 vaccination mandates are a crucial step toward controlling the pandemic, protecting public health, and preventing further loss of life. The evidence overwhelmingly supports their effectiveness, and while concerns about personal freedoms are valid, they must be weighed against the greater good of society. It is our responsibility to take collective action to combat this global crisis and move toward a safer, healthier future. |
Step 9: Revise and Proofread
Edit your essay for clarity, coherence, grammar, and spelling errors. Ensure that your argument flows logically.
Step 10: Cite Your Sources
Include proper citations and a bibliography page to give credit to your sources.
Remember to adjust your approach and arguments based on your target audience and the specific angle you want to take in your persuasive essay about COVID-19.

Paper Due? Why Suffer? That's our Job!
Examples of Persuasive Essay About COVID-19
When writing a persuasive essay about the COVID-19 pandemic, it’s important to consider how you want to present your argument. To help you get started, here are some example essays for you to read:
|
Here is another example explaining How COVID-19 has changed our lives essay:
The COVID-19 pandemic, which began in late 2019, has drastically altered the way we live. From work and education to social interactions and healthcare, every aspect of our daily routines has been impacted. Reflecting on these changes helps us understand their long-term implications.
COVID-19, caused by the novel coronavirus SARS-CoV-2, is an infectious disease first identified in December 2019 in Wuhan, China. It spreads through respiratory droplets and can range from mild symptoms like fever and cough to severe cases causing pneumonia and death. The rapid spread and severe health impacts have led to significant public health measures worldwide.
The pandemic shifted many to remote work and online education. While some enjoy the flexibility, others face challenges like limited access to technology and blurred boundaries between work and home.
Social distancing and lockdowns have led to increased isolation and mental health issues. However, the pandemic has also fostered community resilience, with people finding new ways to connect and support each other virtually.
Healthcare systems have faced significant challenges, leading to innovations in telemedicine and a focus on public health infrastructure. Heightened awareness of hygiene practices, like handwashing and mask-wearing, has helped reduce the spread of infectious diseases.
COVID-19 has caused severe economic repercussions, including business closures and job losses. While governments have implemented relief measures, the long-term effects are still uncertain. The pandemic has also accelerated trends like e-commerce and contactless payments.
The reduction in travel and industrial activities during lockdowns led to a temporary decrease in pollution and greenhouse gas emissions. This has sparked discussions about sustainable practices and the potential for a green recovery.
COVID-19 has reshaped our lives in numerous ways, affecting work, education, social interactions, healthcare, the economy, and the environment. As we adapt to this new normal, it is crucial to learn from these experiences and work towards a more resilient and equitable future. |
Let’s look at another sample essay:
The COVID-19 pandemic has been a transformative event, reshaping every aspect of our lives. In my opinion, while the pandemic has brought immense challenges, it has also offered valuable lessons and opportunities for growth. One of the most striking impacts has been on our healthcare systems. The pandemic exposed weaknesses and gaps, prompting a much-needed emphasis on public health infrastructure and the importance of preparedness. Innovations in telemedicine and vaccine development have been accelerated, showing the incredible potential of scientific collaboration. Socially, the pandemic has highlighted the importance of community and human connection. While lockdowns and social distancing measures increased feelings of isolation, they also fostered a sense of solidarity. People found creative ways to stay connected and support each other, from virtual gatherings to community aid initiatives. The shift to remote work and online education has been another significant change. This transition, though challenging, demonstrated the flexibility and adaptability of both individuals and organizations. It also underscored the importance of digital literacy and access to technology. Economically, the pandemic has caused widespread disruption. Many businesses closed, and millions lost their jobs. However, it also prompted a reevaluation of business models and work practices. The accelerated adoption of e-commerce and remote work could lead to more sustainable and efficient ways of operating in the future. In conclusion, the COVID-19 pandemic has been a profound and complex event. While it brought about considerable hardship, it also revealed the strength and resilience of individuals and communities. Moving forward, it is crucial to build on the lessons learned to create a more resilient and equitable world. |
Check out some more PDF examples below:
Persuasive Essay About Covid-19 Pandemic
Sample Of Persuasive Essay About Covid-19
Persuasive Essay About Covid-19 In The Philippines - Example
If you're in search of a compelling persuasive essay on business, don't miss out on our “ persuasive essay about business ” blog!
Examples of Persuasive Essay About COVID-19 Vaccine
Covid19 vaccines are one of the ways to prevent the spread of COVID-19, but they have been a source of controversy. Different sides argue about the benefits or dangers of the new vaccines. Whatever your point of view is, writing a persuasive essay about it is a good way of organizing your thoughts and persuading others.
A persuasive essay about the COVID-19 vaccine could consider the benefits of getting vaccinated as well as the potential side effects.
Below are some examples of persuasive essays on getting vaccinated for Covid-19.
Covid19 Vaccine Persuasive Essay
Persuasive Essay on Covid Vaccines
Interested in thought-provoking discussions on abortion? Read our persuasive essay about abortion blog to eplore arguments!
Examples of Persuasive Essay About COVID-19 Integration
Covid19 has drastically changed the way people interact in schools, markets, and workplaces. In short, it has affected all aspects of life. However, people have started to learn to live with Covid19.
Writing a persuasive essay about it shouldn't be stressful. Read the sample essay below to get an idea for your own essay about Covid19 integration.
Persuasive Essay About Working From Home During Covid19
Searching for the topic of Online Education? Our persuasive essay about online education is a must-read.
Examples of Argumentative Essay About Covid 19
Covid-19 has been an ever-evolving issue, with new developments and discoveries being made on a daily basis.
Writing an argumentative essay about such an issue is both interesting and challenging. It allows you to evaluate different aspects of the pandemic, as well as consider potential solutions.
Here are some examples of argumentative essays on Covid19.
Argumentative Essay About Covid19 Sample
Argumentative Essay About Covid19 With Introduction Body and Conclusion
Looking for a persuasive take on the topic of smoking? You'll find it all related arguments in out Persuasive Essay About Smoking blog!
Examples of Persuasive Speeches About Covid-19
Do you need to prepare a speech about Covid19 and need examples? We have them for you!
Persuasive speeches about Covid-19 can provide the audience with valuable insights on how to best handle the pandemic. They can be used to advocate for specific changes in policies or simply raise awareness about the virus.
Check out some examples of persuasive speeches on Covid-19:
Persuasive Speech About Covid-19 Example
Persuasive Speech About Vaccine For Covid-19
You can also read persuasive essay examples on other topics to master your persuasive techniques!
Tips to Write a Persuasive Essay About Covid-19
Writing a persuasive essay about COVID-19 requires a thoughtful approach to present your arguments effectively.
Here are some tips to help you craft a compelling persuasive essay on this topic:
- Choose a Specific Angle: Narrow your focus to a specific aspect of COVID-19, like vaccination or public health measures.
- Provide Credible Sources: Support your arguments with reliable sources like scientific studies and government reports.
- Use Persuasive Language: Employ ethos, pathos, and logos , and use vivid examples to make your points relatable.
- Organize Your Essay: Create a solid persuasive essay outline and ensure a logical flow, with each paragraph focusing on a single point.
- Emphasize Benefits: Highlight how your suggestions can improve public health, safety, or well-being.
- Use Visuals: Incorporate graphs, charts, and statistics to reinforce your arguments.
- Call to Action: End your essay conclusion with a strong call to action, encouraging readers to take a specific step.
- Revise and Edit: Proofread for grammar, spelling, and clarity, ensuring smooth writing flow.
- Seek Feedback: Have someone else review your essay for valuable insights and improvements.
Tough Essay Due? Hire Tough Writers!
Common Topics for a Persuasive Essay on COVID-19
Here are some persuasive essay topics on COVID-19:
- The Importance of Vaccination Mandates for COVID-19 Control
- Balancing Public Health and Personal Freedom During a Pandemic
- The Economic Impact of Lockdowns vs. Public Health Benefits
- The Role of Misinformation in Fueling Vaccine Hesitancy
- Remote Learning vs. In-Person Education: What's Best for Students?
- The Ethics of Vaccine Distribution: Prioritizing Vulnerable Populations
- The Mental Health Crisis Amidst the COVID-19 Pandemic
- The Long-Term Effects of COVID-19 on Healthcare Systems
- Global Cooperation vs. Vaccine Nationalism in Fighting the Pandemic
- The Future of Telemedicine: Expanding Healthcare Access Post-COVID-19
In search of more inspiring topics for your next persuasive essay? Our persuasive essay topics blog has plenty of ideas!
To sum it up,
You have read good sample essays and got some helpful tips. You now have the tools you needed to write a persuasive essay about Covid-19. So don't let the doubts stop you, start writing!
If you need professional writing help, don't worry! We've got that for you as well.
MyPerfectWords.com is a professional persuasive essay writing service that can help you craft an excellent persuasive essay on Covid-19. Our experienced essay writer will create a well-structured, insightful paper in no time!
So don't hesitate and place your ' write my essay online ' request today!
Frequently Asked Questions
What is a good title for a covid-19 essay.
A good title for a COVID-19 essay should be clear, engaging, and reflective of the essay's content. Examples include:
- "The Impact of COVID-19 on Global Health"
- "How COVID-19 Has Transformed Our Daily Lives"
- "COVID-19: Lessons Learned and Future Implications"
How do I write an informative essay about COVID-19?
To write an informative essay about COVID-19, follow these steps:
- Choose a specific focus: Select a particular aspect of COVID-19, such as its transmission, symptoms, or vaccines.
- Research thoroughly: Gather information from credible sources like scientific journals and official health organizations.
- Organize your content: Structure your essay with an introduction, body paragraphs, and a conclusion.
- Present facts clearly: Use clear, concise language to convey information accurately.
- Include visuals: Use charts or graphs to illustrate data and make your essay more engaging.
How do I write an expository essay about COVID-19?
To write an expository essay about COVID-19, follow these steps:
- Select a clear topic: Focus on a specific question or issue related to COVID-19.
- Conduct thorough research: Use reliable sources to gather information.
- Create an outline: Organize your essay with an introduction, body paragraphs, and a conclusion.
- Explain the topic: Use facts and examples to explain the chosen aspect of COVID-19 in detail.
- Maintain objectivity: Present information in a neutral and unbiased manner.
- Edit and revise: Proofread your essay for clarity, coherence, and accuracy.

Write Essay Within 60 Seconds!

Caleb S. has been providing writing services for over five years and has a Masters degree from Oxford University. He is an expert in his craft and takes great pride in helping students achieve their academic goals. Caleb is a dedicated professional who always puts his clients first.

Paper Due? Why Suffer? That’s our Job!
Keep reading


An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Elsevier - PMC COVID-19 Collection
The impact of COVID-19 on student experiences and expectations: Evidence from a survey ☆
Esteban m. aucejo.
a Department of Economics, Arizona State University, CEP & NBER, United States of America
Jacob French
b Department of Economics, Arizona State University, United States of America
Maria Paola Ugalde Araya
Basit zafar.
c Department of Economics, University of Michigan, & NBER, United States of America
In order to understand the impact of the COVID-19 pandemic on higher education, we surveyed approximately 1500 students at one of the largest public institutions in the United States using an instrument designed to recover the causal impact of the pandemic on students' current and expected outcomes. Results show large negative effects across many dimensions. Due to COVID-19: 13% of students have delayed graduation, 40% have lost a job, internship, or job offer, and 29% expect to earn less at age 35. Moreover, these effects have been highly heterogeneous. One quarter of students increased their study time by more than 4 hours per week due to COVID-19, while another quarter decreased their study time by more than 5 hours per week. This heterogeneity often followed existing socioeconomic divides. Lower-income students are 55% more likely than their higher-income peers to have delayed graduation due to COVID-19. Finally, we show that the economic and health related shocks induced by COVID-19 vary systematically by socioeconomic factors and constitute key mediators in explaining the large (and heterogeneous) effects of the pandemic.
- • Due to COVID: 13% of students delayed graduation, 40% lost a job, internship, or offer, and 29% expect to earn less at 35.
- • The effects of the pandemic have been highly heterogeneous.
- • Lower-income students are 55% more likely than their higher-income peers to have delayed graduation due to COVID-19.
- • COVID-19's economic and health shocks vary by socioeconomic status and act as key mediators explaining pandemic's effects.
1. Introduction
The disruptive effects of the COVID-19 outbreak have impacted almost all sectors of our society. Higher education is no exception. Anecdotal evidence paints a bleak picture for both students and universities. According to the American Council on Education, enrollment is likely to drop by 15% in the fall of 2020, while at the same time many institutions may have to confront demands for large tuition cuts if classes remain virtual. 1 In a similar vein, students face an increasingly uncertain environment, where financial and health shocks (for example, lack of resources to complete their studies or fear of becoming seriously sick), along with the transition to online learning may have affected their academic performance, educational plans, current labor market participation, and expectations about future employment.
This paper attempts to shed light on the impact of the COVID-19 pandemic on college students. First, we describe and quantify the causal effects of the COVID-19 outbreak on a wide set of students' outcomes/expectations. In particular, we analyze enrollment and graduation decisions, academic performance, major choice, study and social habits, remote learning experiences, current labor market participation, and expectations about future employment. Second, we study how these effects differ along existing socioeconomic divides and whether the pandemic has exacerbated existing inequalities. Finally, we present suggestive evidence on the mechanisms behind the heterogeneous COVID-19 effects by quantifying the relationship between individual-level (financial and health) shocks and students' academic decisions and labor market expectations.
For this purpose, we surveyed about 1500 undergraduate students at Arizona State University (ASU), one of the largest public universities in the United States, in late April 2020. The survey was explicitly designed to not only collect student outcomes and expectations after the onset of the pandemic, but also to recover counterfactual outcomes in the absence of the outbreak. Specifically, the survey asked students about their current experiences/expectations and what those experiences/expectations would have been had it not been for the pandemic. Because we collect information conditional on both states of the world (with the COVID-19 pandemic, and without) from each student , we can directly analyze how each student believes COVID-19 has impacted their current and future outcomes. 2 For example, by asking students about their current GPA in a post-COVID-19 world and their expected GPA in the absence of COVID-19, we can back out the subjective treatment effect of COVID-19 on academic performance. The credibility of our approach depends on: (1) students having well-formed beliefs about outcomes in the counterfactual scenario. This is a plausible assumption in our context since the counterfactual state is a realistic and relevant one - it was the status quo less than two months before the survey, and (2) there being no systematic bias in the reporting of the data - an assumption that is implicitly made when using any survey data. 3
Our findings on academic outcomes indicate that COVID-19 has led to a large number of students delaying graduation (13%), withdrawing from classes (11%), and intending to change majors (12%). Moreover, approximately 50% of our sample separately reported a decrease in study hours and in their academic performance. Predicting the longer-term impact of the pandemic on student achievement is more difficult, but students reported that they expect to take a break from college in the fall 2020 semester at more than twice the rate in previous years. Historically, 28% of students who fail to re-enroll do not return to ASU or another university after 5 years (authors' calculations from ASU first-time freshmen transcript data for the 2012–2014 spring semesters), suggesting that the pandemic may have a lasting impact on the educational achievement of current students. We also find that students report a decreased preference for online instruction as a result of their recent experiences.
As expected, the COVID-19 outbreak also had large negative effects on students' current labor market participation and expectations about post-college labor outcomes. Working students suffered a 31% decrease in their wages and a 37% drop in weekly hours worked, on average. Moreover, around 40% of students lost a job, internship, or a job offer, and 61% reported to have a family member that experienced a reduction in income. The pandemic also had a substantial impact on students' expectations about their labor market prospects post-college. For example, their perceived probability of finding a job before graduation decreased by almost 20%, and their expected earnings when 35 years old (around 15 years from the outbreak) declined by approximately 2.5%. This last finding suggests that students expect the pandemic to have a long-lasting impact on their labor market prospects, which is qualitatively consistent with the literature on graduating during a recession. For instance, Oreopoulos et al. (2012) and Schwandt and von Wachter (2019) find significant reductions in earnings 5 and 10 years after graduation, respectively, and Kahn (2010) finds an even longer-lasting effect on wages. On the other hand, although we are measuring the probability of finding a job before graduating, not unemployment directly, our estimated quantitative effect on students' expectations of finding a job seems to be larger relative to the literature ( Kahn, 2010 ; Altonji et al., 2016 ; and Rothstein, 2020 ).
The data also show that while all subgroups of the population have experienced negative effects due to the outbreak, the size of the effects are heterogeneous. For example, compared to their more affluent peers, lower-income students are 55% more likely to delay graduation due to COVID-19 and are 41% more likely to report that COVID-19 impacted their major choice. Further, COVID-19 nearly doubled the gap between higher- and lower-income students' expected GPA. 4 There also is substantial variation in the pandemic's effect on preference for online learning, with Honors students and males revising their preferences down more than 2.5 times as much as their peers. However, despite appearing to be more disrupted by the switch to online learning, the impact of COVID-19 on Honors students' academic outcomes is consistently smaller than the impact on non-Honors students.
Finally, we evaluate the extent to which mitigating factors associated with more direct economic and health shocks from the pandemic (for example, a family member losing income due to COVID-19, or the expected probability of hospitalization if contracting COVID-19) can explain the heterogeneity in pandemic effects. We find that both types of shock (economic and health) are systematically correlated with students' COVID-19 experiences. For example, the expected probability of delaying graduation due to COVID-19 increases by approximately 25% if either a student's subjective probability of being late on a debt payment in the following 90 days (a measure of financial fragility) or subjective probability of requiring hospitalization conditional on contracting COVID-19 increases by one standard deviation. As expected, the magnitude of health and economic shocks are not homogeneous across the student population. The average of the principal component for the economic and health shocks is about 0.3–0.4 standard deviations higher for students from lower-income families. Importantly, we find that the disparate economic and health impacts of COVID-19 can explain 40% of the delayed graduation gap (as well as a substantial part of the gap for other outcomes) between lower- and higher-income students. This analysis should be viewed as descriptive in nature and not necessarily causal, since omitted factors that are correlated both with the shocks and the outcomes may be driving these relationships.
To our knowledge, this is the first paper to shed light on the effects of COVID-19 on college students' experiences. The treatment effects that we find are large in economic terms. Whether students are overreacting in their response to the COVID-19 shock is not clear. We do find that previous cumulative GPA is a strong predictor of expected semester GPA without COVID-19, suggesting that students' reported expectations are meaningful. However, we know that individuals generally tend to overweight recent experiences ( Malmendier and Nagel, 2016 ; Kuchler and Zafar, 2019 ). Whether students' subjective treatment effects are “correct” in some ex-post sense is beside the point. As long as students are reporting their subjective beliefs without any systematic bias, it is the perceived treatment effects, not actual ones, – regardless of whether they are correct or not – which are fundamental to understanding choices. For example, if students (rightly or wrongly) perceive a negative treatment effect of COVID-19 on the returns to a college degree, this belief will have an impact on their future human capital decisions (such as continuing with their education, choice of major, etc.).
Our results underscore the fact that the COVID-19 shock is likely to exacerbate socioeconomic disparities in higher education. This is consistent with findings regarding the impacts of COVID-19 on K-12 students. Kuhfeld et al. (2020) project that school closures are likely to lead to significant learning losses in math and reading. However, they estimate heterogeneous effects, and conclude that high-performing students are likely to make gains. Likewise, Chetty et al. (2020) find that, post-COVID, student progress on an online math program decreased significantly more in poorer ZIP codes. Our analysis reveals that the heterogeneous economic and health burden imposed by COVID-19 can partially explain these varying impacts. This suggests that by addressing the economic and health impacts imposed by COVID-19, policy makers may be able to prevent COVID-19 from widening existing gaps in higher education.
2.1. Survey
Our data come from an original survey of undergraduate students at Arizona State University (ASU), one of the largest public universities in the United States. Like other higher educational institutions in the US, the Spring 2020 semester started in person. However, in early March during spring break, the school announced that instruction would be transitioned online and that students were advised not to return to campus.
The study was advertised on the My ASU website, accessible only through the student's ASU ID and password. Undergraduate students were invited to participate in an online survey about their experiences and expectations in light of the COVID-19 pandemic, for which they would be paid $10. The study was posted during the second to last week of instruction for the spring semester (April 23rd). Our sample size was constrained by the research funds to 1500 students, and the survey was closed once the desired sample size was reached, which happened within 3 days of posting the survey.
The survey was programmed in Qualtrics. It collected data on students' demographics and family background, their current experiences (both for academic outcomes and non-academic outcomes), and their future expectations. Importantly for the purposes of this study, the survey collected data on what these outcomes/expectations would have been in the counterfactual state, without COVID-19. The survey instrument (with only the relevant sections) can be found here .
2.2. Sample
A total of 1564 respondents completed the survey. 5 90 respondents were ineligible for the study (such as students enrolled in graduate degree programs or diploma programs) and were dropped from the sample. Finally, responses in the 1st and 99th percentile of survey duration were further excluded, leading to a final sample size of 1446. The survey took 38 min to complete, on average (median completion time was 26 min).
The first five columns of Table 1 show how our sample compares with the broader ASU undergraduate population and the average undergraduate student at other large flagship universities (specifically, the largest public universities in each state). Relative to the ASU undergraduate population, our sample has a significantly higher proportion of first-generation students (that is, students with no parent with a college degree), and a smaller proportion of international students. The demographic composition of our sample compares reasonably well with that of students in flagship universities. Our sample is also positively selected in terms of SAT/ACT scores relative to these two populations. The sample may also differ from the student body at other large public schools in that 30% report living on campus, which is not always the norm at other large institutions and may play an important role in how disruptive the pandemic has been. 6
Summary statistics.
| Survey | ASU | P-value | Flagship | P-value | Survey | P-value | Top-10 | P-value | |
|---|---|---|---|---|---|---|---|---|---|
| All | (1)–(2) | Univ. | (1)-(4) | Honors | (6)-(2) | Univ. | (6)-(8) | ||
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | |
| Female | 0.50 | 0.48 | 0.04 | 0.50 | 0.77 | 0.51 | 0.31 | 0.50 | 0.90 |
| Black | 0.04 | 0.04 | 0.15 | 0.07 | 0.00 | 0.02 | 0.00 | 0.07 | 0.00 |
| White | 0.61 | 0.49 | 0.00 | 0.61 | 0.82 | 0.60 | 0.00 | 0.39 | 0.00 |
| Hispanic | 0.20 | 0.24 | 0.00 | 0.12 | 0.00 | 0.12 | 0.00 | 0.12 | 0.76 |
| Int. students | 0.02 | 0.09 | 0.00 | 0.06 | 0.00 | 0.01 | 0.00 | 0.12 | 0.00 |
| First generation , | 0.38 | 0.28 | 0.00 | – | – | 0.20 | 0.00 | – | – |
| Family income , | 97 | 111 | 0.00 | – | – | 117 | 0.07 | – | – |
| Freshman | 0.24 | 0.27 | 0.01 | – | – | 0.29 | 0.44 | – | – |
| Sophomore | 0.25 | 0.24 | 0.19 | – | – | 0.32 | 0.00 | – | – |
| Junior | 0.28 | 0.22 | 0.00 | – | – | 0.24 | 0.41 | – | – |
| Senior | 0.23 | 0.28 | 0.00 | – | – | 0.16 | 0.00 | – | – |
| SAT verbal 25th %tile | 600 | 532 | 0.00 | 557 | 0.00 | 680 | 0.00 | 716 | 0.00 |
| SAT verbal 75th %tile | 720 | 644 | 0.00 | 655 | 0.00 | 750 | 0.00 | 782 | 0.00 |
| SAT math 25th %tile | 600 | 542 | 0.00 | 563 | 0.00 | 690 | 0.00 | 731 | 0.00 |
| SAT math 75th %tile | 740 | 661 | 0.00 | 675 | 0.00 | 780 | 0.00 | 798 | 0.00 |
| ACT 25th %tile | 25 | 22 | 0.00 | 24 | 0.00 | 29 | 0.00 | 32 | 0.00 |
| ACT 75th %tile | 32 | 28 | 0.00 | 29 | 0.00 | 34 | 0.00 | 35 | 0.00 |
| 1446 | 60,108 | 1,339,304 | 322 | 81,118 | |||||
Notes: Data in columns (2), (3) and (8) is from IPEDS 2018. The flagship universities are the 4-year public universities with the highest number of undergraduate students in each state. Means for these columns are weighted by total number of undergraduates in each institution. ACT and SAT data are weighted averages of 2018–2015 years from IPEDS. P -value columns show the p -value of a difference in means test between the two columns indicated by the numbers in the heading.
The better performance on admission tests could be explained by the high proportion of Honors students in our sample (22% compared to 18% in the ASU population). The last four columns of Table 1 show how Honors students compare with ASU students and the average college student at a top-10 university. We see that they perform better than the average ASU student (which is expected) and just slightly worse than the average college student at a top-10 university. The share of white Honors students in our sample (60%) is higher than the proportion in the ASU population and much higher than the proportion of white students in the top-10 universities.
Overall, we believe our sample of ASU students is a reasonable representation of students at other large public schools, while the Honors students may provide insight into the experiences of students at more elite Institutions. Though, it is important to acknowledge that elite institutions may have additional resources to address a global pandemic.
3. Analytic framework
We next outline a simple analytic framework that guides the empirical analysis. Let O i ( COVID – 19) be the potential outcome of individual i associated with COVID-19 treatment. We are interested in the causal impact of COVID-19 on student outcomes:
where the first term on the right-hand side is student i 's outcome in the state of the world with COVID-19, and the second term being student i 's outcome in the state of the world without COVID-19. Recovering the treatment effect at the individual level entails comparison of the individual's outcomes in two alternate states of the world. With standard data on realizations, a given individual is observed in only one state of the world (in our case, COVID – 19 = 1). The alternate outcomes are counterfactual and unobserved. A large econometric and statistics literature studies how to identify these counterfactual outcomes and moments of the counterfactual outcomes (such as average treatment effects) from realized choice data (e.g., Heckman and Vytlacil, 2005 ; Angrist and Pischke, 2009 ; Imbens and Rubin, 2015 ). Instead, the approach we use in this paper is to directly ask individuals for their expected outcomes in both states of the world. From the collected data, we can then directly calculate the individual-level subjective treatment effect. As an example, consider beliefs about end-of-semester GPA. The survey asked students “ What semester-level GPA do you expect to get at the end of this semester ?” This is the first-term on the right-hand side of Eq. (1) . The counterfactual is elicited as follows “ Were it not for the COVID-19 pandemic , what semester-level GPA would you have expected to get at the end of the semester ?”. The difference in the responses to these two questions gives us the subjective expected treatment effect of COVID-19 on the student's GPA. For certain binary outcomes in the survey, we directly ask students for the Δ i . For example, regarding graduation plans, we simply ask a student if the Δ i is positive, negative, or zero: “ How has the COVID-19 pandemic affected your graduation plan ? [ graduate later ; graduation plan unaffected ; graduate earlier ].”
The approach we use in this paper follows a small and growing literature that uses subjective expectations to understand decision-making under uncertainty. Specifically, Arcidiacono et al. (2020) and Wiswall and Zafar (2020) ask college students about their beliefs for several outcomes associated with counterfactual choices of college majors, and estimate the ex-ante treatment effects of college majors on career and family outcomes. Shapiro and Giustinelli (2019) use a similar approach to estimate the subjective ex-ante treatment effects of health on labor supply. There is one minor distinction from these papers: while these papers elicit ex-ante treatment effects, in our case, we look at outcomes that have been observed (for example, withdrawing from a course during the semester) as well as those that will be observed in the future (such as age 35 earnings). Thus, some of our subjective treatment effects are ex-post in nature while others are ex-ante.
The soundness of our approach depends on a key assumption that students have well-formed expectations for outcomes in both the realized state and the counterfactual state. Since the outcomes we ask about are absolutely relevant and germane to students, they should have well-formed expectations for the realized state. In addition, given that the counterfactual state is the one that had been the status quo in prior semesters (and so students have had prior experiences in that state of the world), their ability to have expectations for outcomes in the counterfactual state should not be a controversial assumption. 7 As evidence that students' expectations exhibit meaningful variation, Appendix Fig. A1 shows that previous cumulative GPA is a strong predictor of expected semester GPA with COVID-19.
4. Empirical analysis
4.1. treatment effects.
We start with the analysis of the aggregate-level treatment effects, which are presented in Table 2 . The outcomes are organized in two groups, academic and labor market (see Appendix Table A1 for a complete list of outcomes). The first two columns of the table show the average beliefs for those outcomes where the survey elicited beliefs in both states of the world. The average treatment effects shown in column (3) are of particular interest. Since we can compute the individual-level treatment effects, columns (4)–(7) of the table show the cross-sectional heterogeneity in the treatment effects.
Subjective treatment effects.
| With | Without | Prop. | Prop. | 25th | 75th | ||
|---|---|---|---|---|---|---|---|
| COVID-19 | COVID-19 | >0 | =0 | %tile | %tile | ||
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | |
| Likelihood of taking online classes | 0.46 | 0.50 | −0.04 | 0.31 | 0.22 | −0.20 | 0.08 |
| (0.30) | (0.33) | (0.26) | |||||
| Semester GPA | 3.48 | 3.65 | −0.17 | 0.07 | 0.41 | −0.30 | 0.00 |
| (0.37) | (0.50) | (0.33) | |||||
| Weekly study hours | 15.12 | 16.03 | −0.91 | 0.33 | 0.20 | −5.00 | 4.00 |
| (10.21) | (11.55) | (8.15) | |||||
| Delayed graduation (0/1) | 0.13 | 0.00 | 0.00 | ||||
| (0.34) | |||||||
| Withdraw from a class (0/1) | 0.11 | 0.00 | 0.00 | ||||
| (0.31) | |||||||
| Change major (0/1) | 0.12 | 0.00 | 0.00 | ||||
| (0.33) | |||||||
| Lost in-college job (0/1) | 0.29 | 0.00 | 1.00 | ||||
| (0.45) | |||||||
| In-college weekly hours worked | 12.97 | 24.38 | −11.64 | 0.40 | 0.21 | −22.00 | 0.00 |
| (13.71) | (15.30) | (16.09) | |||||
| In-college weekly earnings , | 147.73 | 237.02 | −21.27 | 0.09 | 0.52 | −1.00 | 0.00 |
| (366.62) | (342.91) | (170.05) | |||||
| Fam. lost job or reduce income (0/1) | 0.61 | 0.00 | 1.00 | ||||
| (0.49) | |||||||
| Lost job offer or internship (0/1) | 0.13 | 0.00 | 0.00 | ||||
| (0.34) | |||||||
| Probability of finding a Job | 55.97 | 69.36 | −13.39 | 0.13 | 0.24 | −20.00 | 0.00 |
| (25.07) | (28.04) | (20.27) | |||||
| Reservation waged | 48.53 | 50.53 | −1.91 | 0.09 | 0.63 | −0.08 | 0.00 |
| (21.95) | (21.93) | (28.02) | |||||
| Expected earnings at 35 years old | 88.18 | 91.49 | −2.34 | 0.06 | 0.65 | −0.07 | 0.00 |
| (33.92) | (33.90) | (28.64) | |||||
Notes: Δ : change. Prop. Δ >0: proportion of students for whom the individual level Δ is positive. Prop. Δ =0: proportion of students for whom the individual level Δ is zero. 25th and 75th percentiles of the cross-sectional distribution of Δ . Standard deviation in parentheses. ( ∗ : p <0.1, ∗∗ : p <0.05, ∗∗∗ : p <0.01).
We see that the average treatment effects are statistically and economically significant for all outcomes. The average impacts on academic outcomes, shown in Panel A, are mostly negative. For example, the average subjective treatment effect of COVID-19 on semester-level GPA is a decline of 0.17 points. More than 50% of the students in our sample expect a decrease in their GPA due to the treatment (versus only 7% expecting an increase). Additionally, 13% of the participants delayed their graduation, 11% withdrew from a class during the spring semester, and 12% stated that their major choice was impacted by COVID-19. 8
While almost no students report planning to drop out due to COVID-19, on average they expect to take a break from ASU in the fall 2020 semester at nearly twice the historical rate. Admittedly, the decision to take a break during a pandemic may be different than in more normal times. However, a substantial increase in the share of students failing to continue their studies is concerning, as historically 28% of students who fail to re-enroll for a fall semester do not return to ASU or another university within 5 years.
Regarding the impact of the pandemic on major choice, students who report that COVID-19 impacted their major choice were more likely to be in lower-paying majors before the pandemic; mean pre-COVID major-specific annual earnings were $43,053 ($46,943) for students whose major choice was (not) impacted by COVID-19. 9 Impacted students were also 9.3 percentage points less likely to be in a science, technology, engineering, or math (STEM) major before COVID-19. 10 We are only able to observe pre- and post-COVID major choices for the subset of students who had switched their major by the date of the survey. 11 Within this selected subsample of switchers, students chose to move into higher paying majors, with an average change in first-year earnings of $3,340. These patterns are generally consistent with the finding that students tend to gravitate towards higher-paying majors when exposed to adverse economic conditions when in college ( Blom et al., 2019 ).
An interesting and perhaps unanticipated result reported in Table 2 is that, on average, students are 4 percentage points less likely to opt for online instruction if given the choice between online and in-person instruction due to their experience with online instruction during the pandemic. 12 13 However, there is a substantial amount of variation in terms of the direction of the effect: 31% (47%) of the participants are now more (less) likely to enroll in online classes. We explore this heterogeneity in more detail in the next section, but it seems that prior experience with online classes somewhat ameliorates the negative experience; the average treatment effect for students with prior experience in online classes is a 2.4 percentage points decrease in their likelihood of enrolling in online classes, versus a 9.5 percentage points decline for their counterparts (difference statistically significant at the 0.1% level).
This large variation in the treatment effects of COVID-19 is apparent in several of the other outcomes, such as study hours, where the average treatment effect of COVID-19 on weekly study hours is −0.9 (that is, students spend 0.9 less hours studying per week due to COVID-19). The interquartile range of the across-subject treatment effect demonstrates substantial variation, with the pandemic decreasing study time by 5 hours at the 25th percentile and increasing study time by 4 hours at the 75th.
Overall, these results suggest that COVID-19 represents a substantial disruption to students' academic experiences, and is likely to have lasting impacts through changes in major/career and delayed graduation timelines. Students' negative experiences with online teaching, perhaps due to the abruptness of the transition, also has implications for the willingness of students to take online classes in the future.
Turning to Panel B in Table 2 , we see that students' current and expected labor market outcomes were substantially disrupted by COVID-19. As for the extensive margin of current employment, on average, 29% of the students lost the jobs they were working at prior to the pandemic (67% of the students were working prior to the pandemic), 13% of students had their internships or job offers rescinded, and 61% of the students reported that a close family member had lost their job or experienced an income reduction. The last statistic is in line with findings from other surveys of widespread economic disruption across the US. 14 Respondents experienced an average decrease of 11.5 hours of work per week and a 21% decrease in weekly earnings, although there was no change in weekly earnings for 52% of the sample, which again reflects substantial variation in the effects of COVID-19 across students.
In terms of labor market expectations, on average, students foresee a 13 percentage points decrease in the probability of finding a job by graduation, a reduction of 2% in their reservation wages, and a 2.3% decrease in their expected earnings at age 35.
The significant changes in reservation wages and expected earnings at age 35 demonstrate that students expect the treatment effects of COVID-19 to be long-lasting. Qualitatively, this is broadly consistent with the literature on graduating during recession. Oreopoulos et al. (2012) finds that graduating during a recession in which the unemployment rate increases 5% implies an initial loss in earnings of 9%, that decreases to 4.5% within 5 years and disappears after 10 years for a sample of male college graduates in Canada. Similarly, Schwandt and von Wachter (2019) find a 2.6% reduction in earnings 10 years after graduation for a 3-percentage point increase in unemployment at graduation, and Kahn (2010) finds an even longer-lasting effect on wages.
A large literature has investigated the impact of graduating during recessions on unemployment rates. Kahn (2010) finds that during the 1980's recession, the probability of being employed right after graduation for white males was largely unaffected by economic conditions. Altonji et al. (2016) only find what they term modest impacts. On the other hand, Rothstein (2020) finds that, for 22 to 23-year-olds graduating from college during the Great Recession, the probability of being employed decreases by 0.7 percentage point for every 1 percentage point increase in the unemployment rate. Using the estimates in Rothstein (2020) and the approximate 10 percentage point increase in the unemployment rate during April 2020, a back-of-the-envelope calculation indicates a 7 percentage point reduction in the probability of being employed for the graduating cohort in our sample. We find that students who are graduating in spring or summer 2020 expect a 35 percentage point decline in the likelihood of finding a job before graduation. While it is difficult to precisely map pre-graduation job finding rates to unemployment over the subsequent year, a 7 percentage point increase in unemployment appears low compared to the impact on students' expectations. It could be the case that the literature estimates are not appropriate for a situation as unexpected and different as a global pandemic, where the economic recession goes hand in hand with health concerns. Having said that, it could also be that students are overreacting to the COVID-19 shock. Data that tracks students' expectations and outcomes over time may be able to shed light on this.
4.2. Heterogeneous effects
We next explore demographic heterogeneity in the treatment effects of COVID-19. Fig. 1 plots the average treatment effects across several relevant demographic divisions including gender, race, parental education, and parental income. Honors college status and cohort are also included as interesting dimensions of heterogeneity in the COVID-19 context. The figure shows the impacts for six of the more economically meaningful outcomes from Table 2 (additional outcomes can be found in Appendix Fig. A2 ).

Treatment effects by demographic group.
(a) Delay Graduation due to COVID (0/1)
(b) Semester GPA ( Δ 0–4)
(c) Change major due to COVID (0/1)
(d) Likelihood take online classes ( Δ 0–1)
(e) Probability job before graduate ( Δ 0–1)
(f) Expected earnings at age 35 (Pct. Δ )
Notes: bars denote 90% confidence interval.
At least four patterns of note emerge from Fig. 1 . First, compared to their classmates, students from disadvantaged backgrounds (lower-income students defined as those with below-median parental income, racial minorities, and first-generation students) experienced larger negative impacts for the academic outcomes, as shown in the first three panels of the figure. 15 The trends are most striking for lower-income students, who are 55% more likely to delay graduation due to COVID-19 than their more affluent classmates (0.16 increase in the proportion of those expecting to delay graduation versus 0.10), expect 30% larger negative effects on their semester GPA due to COVID-19, and are 41% more likely to report that COVID-19 impacted their major choice (these differences are statistically significant at the 5% level). For some academic outcomes, COVID-19 had similarly disproportionate effects on nonwhite and first-generation students, with nonwhite students being 70% more likely to report changing their major preference compared to their white peers and first-generation students being 50% more likely to delay their graduation than students with college-educated parents. Thus, while on average COVID-19 negatively impacted several measures of academic achievement for all subgroups, the effects are significantly more pronounced for socioeconomic groups which were predisposed towards worse academic outcomes pre-COVID. 16 The pandemic's widening of existing achievement gaps can be seen directly in students' expected Semester GPA. Without COVID-19, lower-income students expected a 0.052 lower semester GPA than their higher-income peers. With COVID-19, this gap nearly doubles to 0.098. 17
Second, Panel (d) of Fig. 1 shows that the switch to online learning was substantially harder for some demographic groups; for example, men are 7 percentage points less likely to opt for an online version of a course as a result of COVID-19, while women do not have a statistically significant change in their online preferences. We also see that Honors students revise their preferences by more than 2.5 times the amount of non-Honors students. As we show later (in Table 4 ), these gaps persist after controlling for household income, major, and cohort, suggesting that the switch to online learning mid-semester may have been substantially more disruptive for males and Honors students. While the effect of COVID-19 on preferences for online learning looks similar for males and Honors students, our survey evidence indicates that different mechanisms underpin these shifts. Based on qualitative evidence, it appears that Honors students had a negative reaction to the transition to online learning because they felt less challenged, while males were more likely to struggle with the learning methods available through the online platform. 18 One speculative explanation for the gender difference is that consumption value of college amenities is higher for men (however, Jacob et al. (2018) , find little gender difference in willingness to pay for the amenities they consider).
Composition of COVID effects.
| Delay grad due to COVID (0/100) | COVID impact major choice (0/100) | Prob take online classes ( pp) | Prob job before grad ( pp) | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | (11) | (12) | (13) | (14) | (15) | (16) | (17) | (18) | (19) | (20) | |
| Women | 1.80 | 0.82 | 0.20 | −0.12 | −0.09 | 3.01 | 0.08 | −0.53 | −0.71 | −0.69 | 5.61 | 3.45 | 3.65 | 3.73 | 3.70 | −1.23 | −0.64 | −0.50 | −0.31 | −0.36 |
| (1.66) | (2.04) | (2.16) | (2.07) | (2.12) | (1.65) | (2.03) | (2.08) | (2.03) | (2.05) | (1.46) | (1.61) | (1.66) | (1.65) | (1.67) | (0.98) | (1.13) | (1.13) | (1.15) | (1.13) | |
| Lower-income | 4.34 | 3.26 | 3.84 | 2.68 | 3.15 | 3.08 | 1.16 | 1.74 | 0.73 | 1.33 | 1.96 | 1.47 | 1.40 | 1.76 | 1.41 | −0.40 | 0.13 | −0.52 | 0.38 | −0.16 |
| (1.77) | (1.94) | (1.78) | (1.85) | (1.75) | (1.61) | (1.67) | (1.63) | (1.69) | (1.71) | (1.15) | (1.24) | (1.17) | (1.25) | (1.20) | (1.02) | (1.05) | (0.99) | (1.01) | (0.96) | |
| Honors | − 9.00 | − 7.41 | − 7.75 | − 6.59 | − 6.93 | − 6.36 | − 4.55 | − 4.52 | − 3.88 | − 4.09 | − 4.52 | −2.64 | −2.62 | −2.87 | −2.75 | 0.53 | − 2.18 | − 2.11 | − 2.49 | − 2.56 |
| (1.76) | (1.93) | (2.00) | (1.96) | (1.98) | (1.72) | (1.78) | (1.72) | (1.73) | (1.75) | (1.44) | (1.73) | (1.75) | (1.78) | (1.79) | (1.09) | (1.02) | (1.04) | (1.06) | (1.06) | |
| Student Lost Job (0/1) | 3.59 | 4.07 | −1.03 | −0.58 | − 2.78 | − 2.64 | 0.86 | 0.72 | ||||||||||||
| (2.66) | (2.66) | (2.27) | (2.31) | (1.57) | (1.57) | (1.60) | (1.61) | |||||||||||||
| Family Lost Income (0/1) | 2.31 | 1.77 | 1.53 | 1.01 | −1.45 | −1.30 | − 4.35 | − 4.14 | ||||||||||||
| (2.27) | (2.25) | (1.66) | (1.59) | (1.47) | (1.42) | (1.38) | (1.37) | |||||||||||||
| Student Change in Earnings ($) | 0.00 | 0.00 | 0.00 | 0.00 | − 0.01 | − 0.01 | 0.00 | 0.00 | ||||||||||||
| (0.01) | (0.01) | (0.01) | (0.01) | (0.00) | (0.00) | (0.00) | (0.00) | |||||||||||||
| Prob. miss Debt (0–1) | 17.12 | 13.74 | 15.89 | 12.76 | −2.83 | −2.37 | −4.83 | −3.71 | ||||||||||||
| (4.36) | (4.40) | (3.93) | (4.02) | (2.79) | (2.67) | (3.07) | (3.00) | |||||||||||||
| Principal Component | 2.85 | 1.41 | −0.26 | − 1.49 | ||||||||||||||||
| (0.82) | (0.83) | (0.60) | (0.48) | |||||||||||||||||
| Subjective health (1–5, 5 high) | − 2.68 | − 2.33 | −2.20 | −1.89 | 2.91 | 2.71 | 1.51 | 1.34 | ||||||||||||
| (1.26) | (1.30) | (1.40) | (1.33) | (0.96) | (0.96) | (0.87) | (0.83) | |||||||||||||
| Prob. hosp. if catch COVID (0–1) | 12.89 | 11.56 | 10.98 | 9.74 | 0.11 | 0.10 | − 3.99 | − 3.45 | ||||||||||||
| (4.42) | (4.24) | (4.00) | (4.00) | (2.98) | (3.03) | (1.99) | (1.98) | |||||||||||||
| Prob. catch COVID (0–1) | 8.24 | 6.43 | 9.52 | 7.65 | 2.73 | 3.29 | −2.41 | −1.55 | ||||||||||||
| (4.02) | (3.95) | (3.78) | (3.76) | (2.88) | (2.86) | (2.36) | (2.35) | |||||||||||||
| Principal component | 4.32 | 3.90 | − 1.37 | − 1.66 | ||||||||||||||||
| (0.89) | (0.91) | (0.69) | (0.51) | |||||||||||||||||
| Economic proxies | 0.000 | 0.002 | 0.002 | 0.031 | 0.116 | 0.166 | 0.001 | 0.003 | ||||||||||||
| Health Proxies | 0.000 | 0.000 | 0.000 | 0.000 | 0.001 | 0.002 | 0.006 | 0.022 | ||||||||||||
| Major FE | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Cohort FE | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Mean | 12.93 | 12.93 | 12.93 | 12.93 | 12.93 | 12.24 | 12.24 | 12.24 | 12.24 | 12.24 | −4.18 | −4.18 | −4.18 | −4.18 | −4.18 | −13.39 | −13.39 | −13.39 | −13.39 | −13.39 |
| R | 0.020 | 0.163 | 0.164 | 0.178 | 0.172 | 0.012 | 0.194 | 0.198 | 0.206 | 0.199 | 0.021 | 0.153 | 0.157 | 0.160 | 0.152 | 0.001 | 0.237 | 0.230 | 0.243 | 0.237 |
| N | 1446 | 1446 | 1446 | 1446 | 1446 | 1446 | 1446 | 1446 | 1446 | 1446 | 1446 | 1446 | 1446 | 1446 | 1446 | 1380 | 1380 | 1380 | 1380 | 1380 |
Notes: Standard errors in parentheses bootstrapped with 1000 replications. Each column reports results from a separate OLS regression of the dependent variable onto the covariates (row variables). Dependent variables measured in percentage points. ( ∗ : p <0.1, ∗∗ : p <0.05, ∗∗∗ : p <0.01).
The third trend worth highlighting from Fig. 1 is that Honors students were better able to mitigate the negative effect of COVID-19 on their academic outcomes (panels a, b, and c), despite appearing to be more disrupted by the move to online learning (panel d). Honors students report being less than half as likely as non-Honors students to delay graduation and change their major due to COVID-19. Extrapolating from these patterns provides suggestive evidence that academic impacts for students attending elite schools– the group more comparable to these Honors students– are likely to have been small relative to the impacts for the average student at large public schools.
Finally, the last two panels of Fig. 1 present the COVID effect on two labor market expectations and show much less meaningful heterogeneity across demographic groups compared to the academic outcomes in previous panels. This suggests that, while students believe COVID-19 will impact both their academic outcomes and future labor market outcomes, they do not believe there is a strong connection between these domains. Supporting this observation, the individual-specific treatment effect on semester GPA is only weakly correlated with the individual-specific treatment effects on finding a job before graduation (corr = 0.0497, p = 0.065) and expected earnings at 35 (corr = 0.0467, p = 0.077).
The one notable exception to the lack of heterogeneity in panels (e) and (f) of Fig. 1 are seniors, who on average revised their subjective probability of finding a job before graduation three times as much as other cohorts. Appendix Fig. A3 further breaks down the estimated COVID-19 effects by expected year of graduation. Perhaps unsurprisingly, the 2020 cohort expects much larger effects on immediate job market outcomes such as reservation wages and probability of finding a job before graduation. While average expected changes to job market outcomes are noisier for academically younger students, perhaps reflecting additional uncertainty about the longer-term impacts of COVID-19, they appear to anticipate meaningful changes to their future labor market prospects. Conversely, younger students also expected larger disruptions to academic outcomes such as semester GPA and study time.
5. Understanding the heterogeneous effects
This section presents mediation analysis on the drivers of the underlying heterogeneity in the treatment effects. The COVID-19 pandemic serves as both an economic and a health shock. However, these shocks may have been quite heterogeneous across the various groups, and that could partly explain the heterogeneous treatment effects we documented in the previous section.
5.1. Economic and health mediating factors
We proxy for the financial and health shocks due to COVID-19 by relying on a small but relevant set of covariates which capture more fundamental or first-order disruptions from the pandemic. Financial shocks are characterized based on whether a student lost a job due to COVID-19, whether a student's family members lost income due to COVID-19, the change in a student's monthly earnings due to COVID-19, and the likelihood a student will fail to fully meet debt payments in the next 90 days. To measure health shocks, we consider a student's belief about the likelihood that they will be hospitalized if they contract COVID-19, a student's belief about the likelihood that they will have contracted COVID-19 by summer, and a student's subjective health assessment. Finally, in order to summarize the combined effect of each set of proxies, we construct principal component scores as one-dimensional measures of the financial and health shock to students. 19
Table 3 reports summary statistics of the different economic and health proxies by demographic group. Given the results in Fig. 1 , the remainder of the analysis will focus on three socioeconomic divisions: parental income, gender, and Honors college status. Our data indicate that lower-income students faced larger health and economic shocks as compared to their more affluent peers. In particular, they are almost 10 percentage points more likely to expect to default on their debt payments compared to their higher-income counterparts. Additionally, lower-income students are 16 percentage points more likely to have had a close family member experience an income reduction due to COVID-19. Regarding the health proxies, lower-income students rate their health as worse than higher-income students and perceive a higher probability of being hospitalized if they catch the virus. Finally, the differences in economic and health shocks between lower and higher-income students, as summarized by the principle components of the selected proxy variables, are statistically significant.
Summary statistics for economic and health proxies.
| All | Lower | Higher | P-value | Honors | Not | P-value | Female | Male | P-value | |
|---|---|---|---|---|---|---|---|---|---|---|
| Income | Income | (2)–(3) | Honors | (5)–(6) | (8)–(9) | |||||
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | |
| Likelihood default in next 90 days (0–1) | 0.16 | 0.21 | 0.12 | 0.00 | 0.08 | 0.18 | 0.00 | 0.19 | 0.13 | 0.00 |
| (0.26) | (0.29) | (0.23) | (0.19) | (0.28) | (0.29) | (0.24) | ||||
| Student lost job (0/1) | 0.29 | 0.30 | 0.28 | 0.53 | 0.22 | 0.31 | 0.00 | 0.32 | 0.26 | 0.01 |
| (0.45) | (0.46) | (0.45) | (0.41) | (0.46) | (0.47) | (0.44) | ||||
| Family lost job or earnings (0/1) | 0.61 | 0.70 | 0.54 | 0.00 | 0.54 | 0.64 | 0.00 | 0.67 | 0.56 | 0.00 |
| (0.49) | (0.46) | (0.50) | (0.50) | (0.48) | (0.47) | (0.50) | ||||
| Student change in earnings | −89.30 | −95.40 | −84.16 | 0.36 | −49.42 | −100.72 | 0.00 | −107.27 | −71.02 | 0.00 |
| (230.50) | (230.21) | (230.77) | (181.77) | (241.52) | (237.35) | (221.99) | ||||
| 0.00 | 0.19 | −0.16 | 0.00 | −0.37 | 0.10 | 0.00 | 0.17 | −0.18 | 0.00 | |
| (1.28) | (1.27) | (1.26) | (1.07) | (1.31) | (1.30) | (1.23) | ||||
| Subjective health | 3.98 | 3.88 | 4.05 | 0.00 | 4.06 | 3.95 | 0.04 | 3.90 | 4.06 | 0.00 |
| (0.82) | (0.84) | (0.80) | (0.81) | (0.82) | (0.83) | (0.80) | ||||
| Likelihood hospitalized if catch COVID (0–1) | 0.33 | 0.38 | 0.30 | 0.00 | 0.29 | 0.35 | 0.00 | 0.37 | 0.29 | 0.00 |
| (0.28) | (0.29) | (0.27) | (0.26) | (0.29) | (0.29) | (0.27) | ||||
| Likelihood catch COVID-19 by summer (0–1) | 0.30 | 0.30 | 0.30 | 0.75 | 0.29 | 0.31 | 0.17 | 0.32 | 0.29 | 0.01 |
| (0.24) | (0.24) | (0.23) | (0.23) | (0.24) | (0.24) | (0.23) | ||||
| 0.00 | 0.18 | −0.15 | 0.00 | −0.20 | 0.06 | 0.00 | 0.18 | −0.19 | 0.00 | |
| (1.15) | (1.19) | (1.09) | (1.10) | (1.16) | (1.18) | (1.09) | ||||
Notes: P-value columns report the p-value of a difference in means test between the two columns indicated by the numbers in the heading.
Columns (5)–(7) of Table 3 show that both economic and health shocks are larger for non-Honors students. In fact, the average differences in the principal component scores for both the economic and health factors is larger for these two groups than for the income groups. Likewise, the last three columns of the table show that women experienced larger COVID-19 shocks due to economic and health factors. These differences are partly driven by the fact that, in our sample, females are more likely to report that they belong to a lower-income household than males (50% vs. 42%).
In short, Table 3 makes clear that the impacts of COVID-19 on the economic well-being and health of students have been quite heterogeneous, with lower-income and lower-ability students being more adversely affected.
5.2. The role of economic and health shocks on explaining the COVID-19 effects
To investigate the role of economic and health shocks in explaining the heterogeneous treatment effects (in Section 4.2 ), we estimate the following specification:
where Δ i is the COVID-19 treatment effect for outcome O on student i . Demog i is a vector including indicators for gender, lower-income, Honors status, and dummies for cohort year and major. FinShock i and HealthShock i are vectors containing the shock proxies or their principal component. Finally, ε i denotes an idiosyncratic shock.
The parameters of interest are α 2 and α 3 . A causal interpretation of these parameters requires FinShock i and HealthShock i to be independent of ε i . This seems unlikely in our context as unobservables correlated with FinShock i and HealthShock i may also modulate COVID-19's impact on academic outcomes. Therefore, we prefer to interpret α 2 and α 3 as simple correlations. Nevertheless, we believe this descriptive evidence can be informative from a policy perspective.
Table 4 shows estimates of Eq. (2) for four different outcomes ( Appendix Table A2 shows the estimates for additional outcomes). For each outcome, five specifications are reported ranging from controlling for only demographic variables in the first specification to controlling for both economic and health factors in the fourth specification. Finally, the last column includes only the principal component of each shock to provide insight about overall effects, given that certain shock proxies show high levels of correlation (see Appendix Table A4 for the correlations within each set of proxies).
Several important messages emerge from Table 4 . First, both shocks are (economically and statistically) significant correlates of the COVID-19 effects on students' outcomes. In particular, F-tests show that the financial and health shock proxies are jointly significant across almost all specifications. 20 This is also reflected in the statistical significance of the principal components. Moreover, the fact that the effect of key proxy variables remains robust when we simultaneously control for both shocks demonstrates the robustness of our results. For example, we find that a 50 percentage point increase in the probability of being late on debt payments is associated with an increase in the probability of delaying graduation and switching majors due to COVID-19 of 6.9 and 6.4 percentage points respectively. These effects are large given that they represent more than half of the overall COVID-19 treatment effect for these variables. Similarly, we find that an analogous increase in the probability of hospitalization if contracting COVID-19 is associated with a 6 and 5 percentage points increase in the probability of delaying graduation and switching majors due to COVID-19.
Second, in terms of labor market expectations, we find that the change in the expected probability of finding a job before graduation strongly depends on having a family member that lost income (which is also correlated with the student himself losing a job). In particular, the size of this effect represents 32% of the overall COVID-19 treatment effect. Therefore, this finding suggests that students' labor market expectations are driven in large part by personal/family experiences.
Third, although the proxies play an important role in explaining the pandemic's impact on students, there is still a substantial amount of variation in COVID-19 treatment effects left unexplained. Across the four outcomes in Table 4 , the full set of proxies explain less than a quarter of the variation in outcomes across individuals. Appendix Fig. A4 visualizes this variation by plotting the distribution of several continuous outcomes with and without controls. While the interquartile range noticeably shrinks after conditioning on the proxy variables, these plots highlight the large amount of variation in treatment effects remaining after conditioning on the proxies.
Finally, our results show that the financial and health shocks play an important role in explaining the heterogeneous effects of the COVID-19 outbreak. In particular, columns (4) and (9) demonstrate that economic and health factors together can explain approximately 40% and 70% of the income gap in COVID-19's effect on delayed graduation and changing major respectively. The gap between Honors and non-Honors students is likewise reduced by 27% and 39% for the same outcomes. Taken together, these results imply that differences in the magnitude of COVID-19's economic and health impact can explain a significant proportion of the demographic gaps in COVID-19's effect on the decision to delay graduation, the decision to change major, and preferences for online learning. These results are important and suggest that focusing on the needs of students who experienced larger financial or health shocks from COVID-19 may be an effective way to minimize the disparate disruptive effects and prevent COVID-19 from exacerbating existing achievement gaps in higher education.
6. Conclusions
This paper provides the first systematic analysis of the effects of COVID-19 on higher education. To study these effects, we surveyed 1500 students at Arizona State University, and present quantitative evidence showing the negative effects of the pandemic on students' outcomes and expectations. For example, we find that 13% of students have delayed graduation due to COVID-19. Expanding upon these results, we show that the effects of the pandemic are highly heterogeneous, with lower-income students 55% more likely to delay graduation compared to their higher-income counterparts. We further show that the negative economic and health impacts of COVID-19 have been significantly more pronounced for less advantaged groups, and that these differences can partially explain the underlying heterogeneity that we document. Our results suggest that by focusing on addressing the economic and health burden imposed by COVID-19, as measured by a relatively narrow set of mitigating factors, policy makers may be able to prevent COVID-19 from widening existing achievement gaps in higher education.
Declaration of competing interest
The authors declare that they have no relevant or material financial interests that relate to the research described in this paper. There are no declarations of interest.
☆ Noah Deitrick and Adam Streff provided excellent research assistance. All errors that remain are ours.
1 See, the New York Times article “ After Coronavirus , Colleges Worry : Will Students Come Back ?” (April 15, 2020) for a discussion surrounding students' demands for tuition cuts.
2 In some cases, instead of asking students for the outcomes in both states of the world, we directly ask for the difference. For example, the survey asked how the pandemic had affected the student's graduation date.
3 This approach has been used successfully in several other settings, such as to construct career and family returns to college majors ( Arcidiacono et al., 2020 ; Wiswall and Zafar, 2020 ), and the causal impact of health on retirement ( Shapiro and Giustinelli, 2019 ).
4 The income gap in GPA increased from 0.052 to 0.098 on a 4 point scale. It is significant at the 1% level in both scenarios.
5 The 64 people taking the survey at the moment the target sample size (1500) was reached were allowed to finish.
6 59% of Honors students in our sample report living on campus.
7 This is different from asking students in normal times about their expected outcomes in a state with online teaching and no campus activities (COVID-19) since most students would not have had any experience with this counterfactual prior to March this year.
8 Altonji et al. (2016) finds a small but positive effect on the probability of attending graduate school when graduating into a recession. This is suggestive evidence that students try to avoid entering the labor market when economic conditions are adverse. Our results on delayed graduation are consistent with students avoiding entering the labor market at inopportune times.
9 For this calculation, we take earnings data from the US Department of Education College Scorecard dataset. Major-specific earnings are calculated using median first-year earnings for ASU graduates in 2015 and 2016 by two-digit CIP code. Observable earnings averaged within major category.
10 STEM major designation made using two-digit CIP code and The STEM Designated Degree Program from the US Department of Homeland Security.
11 This includes 77 respondents, or 43% of those who say COVID-19 impacted their major choice.
12 The relevant survey question read: “ Suppose you are given the choice to take a course online/remote or in-person . [ Had you NOT had experience with online/remote classes this semester ], what is the percent chance that you would opt for the online/remote option ?”
13 This result is in line with a survey about eLearning experiences across different universities in Washington and New York that concludes that 75% of the students are unhappy with the quality of their classes after moving to online learning due to COVID-19.
14 According to the US Census Bureau Household Pulse Survey Week 3, 48% of the surveyed households have experienced a loss in employment income since March 13 2020.
15 The cutoff for median parental income in our sample is $80,000.
16 Based on analysis of ASU administrative data including transcripts, we find that, relative to their counterparts, first-generation, lower-income, and non-white students drop out at higher rates, take longer to graduate, have lower GPAs at graduation, and are more likely to switch majors when in college (see Appendix Table A3 ).
17 The difference is significant at 1% in both cases.
18 Honors students were as likely as non-Honors students to say that classes got easier after they went online but, conditional on saying classes got easier, were 47% more likely to say “homework/test questions got easier.” Conversely, males were marginally more likely to say classes got harder after they went online (10% more likely, p = 0.055) and, conditional on this, were 14% more likely to say that “online material is not clear”.
19 Eigenvalues indicate the presence of only one principal component for each of the shocks.
20 The only exception is the financial shock when explaining changes in the probability of taking classes online.

Expected and previous academic performance.
Notes: Figure plots mean expected GPA with COVID-19 against students' cumulative GPA up to the spring 2020 semester. The 45 degree line is also plotted for reference.

More treatment effects by demographic group.
(a) Withdrew from Class due to COVID (0/1); (b) Social Events per Week ( Δ 0–14); (c) Move in With Family due to COVID (0/1); (d) Weekly Study Hours ( Δ 0–40); (e) Reservation Wage (Pct. Δ )
Notes: Bars denote 90% confidence interval.

Cohort trends.
Notes: Figure plots average COVID-19 effects for a series of outcomes. The x-axis variable in each panel is expected academic year of graduation (after COVID), with summer graduation dates included in the previous academic year. Bars denote 90% confidence interval.

Distribution of individual effects.
Notes: Data winsorized below 5% and above 95%. Controls include cohort fixed effects, major fixed effects, and the economic/health proxies in Table 3 . Conditional distribution adjusted to preserve unconditional mean. Within each plot: middle line represents median, edges of box represent interquatile range (IQR), edge of whisker represents the adjacent values or the 25th(75th) percentile plus(minus) 1.5 times the IQR. Outlier observations past adjacent values plotted as individual points.
| With | Without | Prop. | Prop. | 25th | 75th | ||
|---|---|---|---|---|---|---|---|
| COVID-19 | COVID-19 | >0 | =0 | %tile | %tile | ||
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | |
| Likelihood of taking online classes | 0.46 (0.33) | 0.50 (0.30) | −0.04 (0.26) | 0.31 | 0.22 | −0.20 | 0.08 |
| Semester GPA | 3.48 (0.50) | 3.65 (0.37) | −0.17 (0.33) | 0.07 | 0.41 | −0.30 | 0.00 |
| Weekly study hours | 15.12 (11.55) | 16.03 (10.21) | −0.91 (8.15) | 0.33 | 0.20 | −5.00 | 4.00 |
| Delayed graduation (0/1) | 0.13 (0.34) | 0.00 | 0.00 | ||||
| Withdraw from a class (0/1) | 0.11 (0.31) | 0.00 | 0.00 | ||||
| Change major (0/1) | 0.12 (0.33) | 0.00 | 0.00 | ||||
| Time in classes | −0.10 (0.87) | 0.33 | 0.24 | −1.00 | 1.00 | ||
| Time studying by myself | 0.28 (0.83) | 0.52 | 0.23 | 0.00 | 1.00 | ||
| Time studying with peers | −0.75 (0.51) | 0.04 | 0.18 | −1.00 | −1.00 | ||
| Lost in-college job (0/1) | 0.29 (0.45) | 0.00 | 1.00 | ||||
| In-college weekly hours worked | 12.97 (15.30) | 24.38 (13.71) | −11.64 (16.09) | 0.40 | 0.21 | −22.00 | 0.00 |
| In-college weekly earnings , | 147.73 (342.91) | 237.02 (366.62) | −21.27 (170.05) | 0.09 | 0.52 | −1.00 | 0.00 |
| Fam. lost job or reduce income (0/1) | 0.61 (0.49) | 0.00 | 1.00 | ||||
| Lost job offer or internship (0/1) | 0.13 (0.34) | 0.00 | 0.00 | ||||
| Probability of finding a Job | 55.97 (28.04) | 69.36 (25.07) | −13.39 (20.27) | 0.13 | 0.24 | −20.00 | 0.00 |
| Reservation waged | 48.53 (21.93) | 50.53 (21.95) | −1.91 (28.02) | 0.09 | 0.63 | −0.08 | 0.00 |
| Expected earnings at 35 years old | 88.18 (33.90) | 91.49 (33.92) | −2.34 (28.64) | 0.06 | 0.65 | −0.07 | 0.00 |
| Time working for pay | −0.46 (0.66) | 0.09 | 0.35 | −1.00 | 0.00 | ||
| Making a lot of money | 0.26 (0.61) | 0.35 | 0.56 | 0.00 | 1.00 | ||
| Being a leader in your line of work | 0.16 (0.55) | 0.24 | 0.68 | 0.00 | 0.00 | ||
| Enjoying your line of work | 0.20 (0.63) | 0.32 | 0.56 | 0.00 | 1.00 | ||
| Family-life Balance | 0.34 (0.63) | 0.42 | 0.49 | 0.00 | 1.00 | ||
| Job security | 0.55 (0.67) | 0.66 | 0.24 | 0.00 | 1.00 | ||
| Have opt. to be helpful to others | 0.38 (0.63) | 0.46 | 0.45 | 0.00 | 1.00 | ||
| Have opt. to work with people | 0.08 (0.68) | 0.28 | 0.53 | 0.00 | 1.00 | ||
| Number of weekly social events | 0.26 (1.28) | 4.44 (3.82) | −4.17 (3.66) | 0.01 | 0.08 | −5.00 | −2.00 |
| Time on social media | 0.62 (0.61) | 0.69 | 0.24 | 0.00 | 1.00 | ||
| Time news and online browsing | 0.71 (0.53) | 0.75 | 0.21 | 1.00 | 1.00 | ||
| Time online entertainment | 0.74 (0.54) | 0.78 | 0.17 | 1.00 | 1.00 | ||
| Time in sports and exercise | −0.46 (0.75) | 0.15 | 0.23 | −1.00 | 0.00 | ||
| Time commuting | −0.89 (0.36) | 0.02 | 0.07 | −1.00 | −1.00 | ||
| Time sleeping | 0.17 (0.83) | 0.44 | 0.28 | −1.00 | 1.00 | ||
Composition of COVID effects: more outcomes.
| Expect earn at age 35 ( pp) | Res wage ( pp) | Sem GPA ( 0–4) | Withdrew class b/c COVID (0/100) | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | (11) | (12) | (13) | (14) | (15) | (16) | (17) | (18) | (19) | (20) | |
| Women | 0.60 | −0.08 | −0.04 | 0.07 | 0.17 | 1.90 | 2.18 | 2.18 | 2.22 | 2.33 | 0.04 | 0.03 | 0.03 | 0.03 | 0.03 | −0.02 | −0.00 | −0.01 | −0.01 | −0.01 |
| (1.35) | (1.48) | (1.62) | (1.58) | (1.66) | (1.47) | (2.47) | (2.59) | (2.61) | (2.60) | (0.02) | (0.02) | (0.02) | (0.02) | (0.02) | (0.02) | (0.02) | (0.02) | (0.02) | (0.02) | |
| Lower-Income | 0.56 | 1.27 | 1.18 | 1.30 | 1.46 | −0.13 | −0.02 | −0.24 | −0.11 | −0.03 | − 0.04 | −0.03 | − 0.05 | −0.03 | − 0.04 | 0.03 | 0.02 | 0.03 | 0.02 | 0.02 |
| (1.62) | (1.62) | (2.11) | (1.65) | (2.11) | (1.35) | (1.58) | (1.62) | (1.77) | (1.55) | (0.02) | (0.02) | (0.02) | (0.02) | (0.02) | (0.02) | (0.02) | (0.02) | (0.02) | (0.02) | |
| Honors | 4.92 | 5.53 | 5.60 | 5.47 | 5.22 | −1.17 | −0.95 | −0.90 | −0.93 | −1.13 | 0.04 | 0.04 | 0.04 | 0.03 | 0.04 | − 0.06 | − 0.06 | − 0.07 | − 0.06 | − 0.06 |
| (3.04) | (3.37) | (3.24) | (3.29) | (3.15) | (1.66) | (1.84) | (1.76) | (1.84) | (1.81) | (0.02) | (0.02) | (0.02) | (0.02) | (0.02) | (0.02) | (0.02) | (0.02) | (0.02) | (0.02) | |
| Student lost job (0/1) | −2.38 | −2.39 | 1.13 | 1.08 | −0.02 | −0.02 | −0.01 | −0.00 | ||||||||||||
| (1.86) | (1.86) | (2.10) | (2.11) | (0.03) | (0.03) | (0.02) | (0.02) | |||||||||||||
| Family lost income (0/1) | − 2.67 | −2.31 | −1.03 | −0.73 | − 0.06 | − 0.05 | 0.02 | 0.01 | ||||||||||||
| (1.43) | (1.48) | (1.91) | (1.93) | (0.02) | (0.02) | (0.02) | (0.02) | |||||||||||||
| Student change in earnings ($) | −0.00 | −0.00 | 0.00 | 0.00 | − 0.00 | −0.00 | −0.00 | −0.00 | ||||||||||||
| (0.00) | (0.00) | (0.00) | (0.00) | (0.00) | (0.00) | (0.00) | (0.00) | |||||||||||||
| Prob. miss debt (0–1) | 2.21 | 3.35 | −1.16 | −0.29 | − 0.13 | − 0.11 | ∗∗0.10 | ∗0.08 | ||||||||||||
| (5.47) | (6.26) | (3.07) | (2.98) | (0.04) | (0.04) | (0.04) | (0.05) | |||||||||||||
| Principal component | −0.69 | −0.28 | − 0.02 | 0.02 | ||||||||||||||||
| (0.49) | (0.57) | (0.01) | (0.01) | |||||||||||||||||
| Subjective health (1–5, 5 high) | 2.30 | 2.31 | 1.24 | 1.25 | 0.04 | 0.04 | − 0.02 | − 0.02 | ||||||||||||
| (1.26) | (1.29) | (0.68) | (0.71) | (0.01) | (0.01) | (0.01) | (0.01) | |||||||||||||
| Prob. hosp. if catch COVID (0–1) | 2.27 | 2.00 | 1.93 | 2.09 | −0.02 | −0.01 | 0.04 | 0.03 | ||||||||||||
| (3.63) | (3.85) | (4.23) | (4.17) | (0.04) | (0.04) | (0.04) | (0.05) | |||||||||||||
| Prob. catch COVID (0–1) | −4.49 | −4.77 | −5.64 | −5.53 | −0.05 | −0.03 | 0.06 | 0.05 | ||||||||||||
| (2.84) | (3.51) | (3.55) | (3.79) | (0.04) | (0.04) | (0.04) | (0.04) | |||||||||||||
| Principal component | −1.13 | −0.72 | − 0.03 | 0.02 | ||||||||||||||||
| (0.86) | (0.71) | (0.01) | (0.01) | |||||||||||||||||
| Economic proxies | 0.267 | 0.304 | 0.702 | 0.767 | 0.000 | 0.000 | 0.045 | 0.101 | ||||||||||||
| Health proxies | 0.244 | 0.290 | 0.104 | 0.172 | 0.000 | 0.003 | 0.010 | 0.039 | ||||||||||||
| Major FE | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Cohort FE | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Mean | −2.34 | −2.34 | −2.34 | −2.34 | −2.34 | −1.91 | −1.91 | −1.91 | −1.91 | −1.91 | −0.17 | −0.17 | −0.17 | −0.17 | −0.17 | 0.11 | 0.11 | 0.11 | 0.11 | 0.11 |
| R | 0.005 | 0.046 | 0.048 | 0.051 | 0.045 | 0.001 | 0.087 | 0.089 | 0.090 | 0.087 | 0.012 | 0.169 | 0.164 | 0.177 | 0.164 | 0.010 | 0.142 | 0.141 | 0.148 | 0.146 |
| N | 1435 | 1435 | 1435 | 1435 | 1435 | 1430 | 1430 | 1430 | 1430 | 1430 | 1446 | 1446 | 1446 | 1446 | 1446 | 1446 | 1446 | 1446 | 1446 | 1446 |
Notes: Standard errors in parentheses bootstrapped with 1000 replications. Each column reports results from a separate OLS regression of the dependent variable onto the covariates (row variables). Dependent variables measured in percentage points (except GPA). ( ∗ : p <0.1, ∗∗ : p <0.05, ∗∗∗ : p <0.01).
Existing achievement gaps.
| Years to graduate | Cum GPA at grad | Graduate | Dropout | Ever switch major | |
|---|---|---|---|---|---|
| Women | 3.37 | 3.39 | 0.62 | 0.22 | 0.54 |
| Men | 3.54 | 3.25 | 0.54 | 0.28 | 0.51 |
| −0.16 | 0.15 | 0.08 | −0.06 | 0.02 | |
| First generation | 3.49 | 3.26 | 0.49 | 0.33 | 0.52 |
| Not first generation | 3.40 | 3.36 | 0.55 | 0.23 | 0.49 |
| 0.10 | −0.10 | −0.06 | 0.10 | 0.03 | |
| Low income | 3.54 | 3.28 | 0.50 | 0.32 | 0.52 |
| High income | 3.30 | 3.37 | 0.57 | 0.20 | 0.48 |
| 0.24 | −0.09 | −0.07 | 0.12 | 0.04 | |
| Nonwhite | 3.51 | 3.25 | 0.55 | 0.29 | 0.54 |
| White | 3.40 | 3.38 | 0.61 | 0.21 | 0.52 |
| 0.11 | −0.13 | −0.06 | 0.08 | 0.02 | |
| Honors | 3.34 | 3.67 | 0.83 | 0.09 | 0.43 |
| Non-honors | 3.47 | 3.25 | 0.55 | 0.27 | 0.54 |
| −0.14 | 0.42 | 0.29 | −0.18 | −0.11 | |
Notes: Sample includes all first time freshman at ASU's main campus who started within the last 10 years. N = 58,426. ( ∗ : p <0.1, ∗∗ : p <0.05, ∗∗∗ : p <0.01).
Correlation of shock proxies.
| Student lost | Family lost | Student | Likelihood | |
| Job | Income | Change in earnings | Default in next 90 days | |
| Student lost job (0/1) | 1.000 | |||
| Family lost income (0/1) | 0.174 | 1.000 | ||
| Student change in earnings ($) | −0.572 | −0.153 | 1.000 | |
| Likelihood default in next 90 days (0–1) | 0.225 | 0.176 | −0.203 | 1.000 |
| Subjective | Likelihood | Likelihood | |
| Health | Hospitalized if catch COVID | Catch COVID by summer | |
| Subjective health (1–5, 5 High) | 1.000 | ||
| Likelihood hospitalized if catch COVID (0–1) | −0.293 | 1.000 | |
| Likelihood catch COVID by summer (0–1) | −0.053 | 0.093 | 1.000 |
Notes: Table reports correlation matrix for indicated variables.
- Altonji J., Arcidiacono P., Maurel A. Handbook of the Economics of Education. vol. 5. Elsevier; Cambridge, MA: 2016. The analysis of field choice in college and graduate school: determinants and wage effects; pp. 305–396. [ Google Scholar ]
- Angrist J.D., Pischke J.-S. Princeton University Press; Princeton: 2009. Mostly Harmless Econometrics: An Empiricist’s Companion. OCLC: ocn231586808. [ Google Scholar ]
- Arcidiacono P., Hotz V.J., Maurel A., Romano T. Ex ante returns and occupational choice. J. Polit. Econ. 2020 (forthcoming) [ Google Scholar ]
- Blom E., Cadena B.C., Keys B.J. 2019. Investment Over the Business Cycle: Insights from College Major Choice. (Working Paper) [ Google Scholar ]
- Chetty R., Friedman J.N., Hendren N., Stepner M. 2020, May. Real-Time Economics: A New Platform to Track the Impacts of COVID-19 on People, Businesses, and Communities Using Private Sector Data. [ Google Scholar ]
- Heckman J.J., Vytlacil E. Structural equations, treatment effects, and econometric policy evaluation. Econometrica. 2005, May; 73 (3):669–738. [ Google Scholar ]
- Imbens G., Rubin D.B. Causal inference: for statistics, social and biomedical sciences: an introduction. OCLC. 2015; 985493948 [ Google Scholar ]
- Jacob B., McCall B., Stange K. College as country club: do colleges cater to students’ preferences for consumption? J. Labor Econ. 2018; 36 (2):40. [ Google Scholar ]
- Kahn L.B. The long-term labor market consequences of graduating from college in a bad economy. Labour Econ. 2010, April; 17 (2):303–316. [ Google Scholar ]
- Kuchler T., Zafar B. Personal experiences and expectations about aggregate outcomes. J. Financ. 2019, October; 74 (5):2491–2542. [ Google Scholar ]
- Kuhfeld M., Soland J., Tarasawa B., Johnson A., Ruzek E., Liu J. 2020, May. Projecting the Potential Impacts of COVID-19 School Closures on Academic Achievement. Publisher: EdWorkingPapers.com. [ Google Scholar ]
- Malmendier U., Nagel S. Learning from inflation experiences *. Q. J. Econ. 2016, February; 131 (1):53–87. [ Google Scholar ]
- Oreopoulos P., von Wachter T., Heisz A. The short- and long-term career effects of graduating in a recession. Am. Econ. J. Appl. Econ. 2012, January; 4 (1):1–29. [ Google Scholar ]
- Rothstein J. 2020, May. The Lost Generation? Labor Market Outcomes for Post Great Recession Entrants. [ Google Scholar ]
- Schwandt H., von Wachter T. Unlucky cohorts: estimating the long-term effects of entering the labor market in a recession in large cross-sectional data sets. J. Labor Econ. 2019; 37 (S1):S161–S198. [ Google Scholar ]
- Shapiro M., Giustinelli P. 2019, July. SeaTE: Subjective ex Ante Treatment Effect of Health on Retirement. [ Google Scholar ]
- Wiswall M., Zafar B. Human capital investments and expectations about career and family. J. Polit. Econ. 2020 (forthcoming) [ Google Scholar ]
- Open access
- Published: 08 June 2021
Impact of COVID-19 on the mental health of US college students
- Jenny Lee 1 ,
- Matthew Solomon 1 ,
- Tej Stead 1 ,
- Bryan Kwon 1 &
- Latha Ganti 2 , 3 , 4
BMC Psychology volume 9 , Article number: 95 ( 2021 ) Cite this article
86k Accesses
127 Citations
72 Altmetric
Metrics details
Background/aim
In the beginning of 2020, the novel Coronavirus disease (COVID-19) caused by the SARS-CoV-2 virus, became a public health emergency in the U.S. and rapidly escalated into a global pandemic. Because the SARS-CoV-2 virus is highly contagious, physical distancing was enforced and indoor public spaces, including schools and educational institutions, were abruptly closed and evacuated to ensure civilian safety. Accordingly, educational institutions rapidly transitioned to remote learning. We investigated the impacts of the COVID-19 pandemic on domestic U.S. college students, ages 18–24 years.
Through Pollfish®’s survey research platform, we collected data from 200 domestic U.S. college students in this age range (N = 200) regarding the physical, emotional, and social impacts of COVID-19 as well as key background information (e.g. whether or not they are first-generation or if they identify with the LGBTQIA+ community).
Our results indicate that students closer to graduating faced increases in anxiety (60.8%), feeling of loneliness (54.1%), and depression (59.8%). Many reported worries for the health of loved ones most impacted their mental health status (20.0%), and the need to take care of family most affected current and future plans (31.8%). Almost one-half of students took to exercising and physical activity to take care of their mental health (46.7%). While a third did not have strained familial relationships (36.5%), almost one half did (45.7%). A majority found it harder to complete the semester at home (60.9%), especially among those who had strained relationships with family (34.1%). Seventy percent spent time during the pandemic watching television shows or movies. Significantly more men, first-generation, and low-income students gained beneficial opportunities in light of the pandemic, whereas their counterparts reported no impact. First-generation students were more likely to take a gap year or time off from school.
Conclusions
Although students found ways to take care of themselves and spent more time at home, the clear negative mental health impacts call for schools and federal regulations to accommodate, support, and make mental health care accessible to all students.
Peer Review reports
Introduction
The outbreak of the SARS-CoV-2 virus, originally from Wuhan, China, in December 2019 gave rise to an ongoing global public health crisis addressing the proliferation of the novel Coronavirus disease (COVID-19). The SARS-CoV-2 virus directly targets the respiratory system in humans with characteristic symptoms of cough, fever, sore throat, dyspnea, and fatigue [ 1 ]. As the virus continued spreading over 2020, more findings on the epidemiological characteristics of SARS-CoV-2 have been divulged to the public. A study showed that the COVID-19 disease presents varying lengths of incubation periods, typically an average of 5.2 days, and it is estimated to have a slightly higher basic reproduction number (2.24–3.58) than that of the original SARS-CoV virus [ 1 ]. According to the National Health Commission of China, the virus can be transmitted through aerosols, droplets, contacts, respiratory aspirates, and feces, with both animals (e.g., bats, pangolins) and humans being veritable modes of transmission [ 2 ]. Accurate and accelerated testing is necessary to control this extremely contagious disease in cities, communities, and hospitals.
Due to the sudden outbreak of COVID-19, most universities across the United States were forced to send their students home early for the 2019–2020 academic year to prevent spread and protect students as well as surrounding communities. The sudden change in students’ learning environment, the quality of their education, and other circumstances caused students to face unique challenges, adversely impacting their mental health. The loss of internships, on-campus jobs, and other opportunities also contributed to the stress and declining mental health of students. According to a study done on a cohort of students attending Dartmouth College, there were noticeable differences in behavioral and mental health over the course of the pandemic thus far, with a higher number of self-reported cases of depression and anxiety around final exams [ 3 ].
Other minority communities also faced particular hardship in light of the pandemic. For example, greater proportions of the lesbian, gay, bisexual, transgender, and queer or questioning (LGBTQ) population do not have access to health insurance and struggle with poverty compared to the non-LGBTQ population [ 4 ]. Because of their health disparities and social disadvantages, the mental health of LGBTQ students is exacerbated due to the psychological trauma that can come with the COVID-19 pandemic. Furthermore, people of color and those in socioeconomically disadvantaged groups are more likely to be mentally overwhelmed due to the unequal burden of finances, illness, and death. In a study done at a hospital in northern California of COVID-19 patients, non-Hispanic African Americans were found to be 2.7 times more likely to be hospitalized compared to non-Hispanic white patients [ 5 ].
A study of college students from India [ 6 ] found that both anxiety and depression were prevalent in their cohort, with women being affected more. They also noted a disturbed sleeping pattern which aligns with both anxiety and depression. A study that used smartphone-based ecological momentary assessments of anxiety and optimism related to COVID-19 and other generic mental health variables 6 times daily [ 7 ] found widespread mental health impact, especially anxiety, in their cohort of 140 students. Yet another study of college students [ 8 ] found a significant decline in physical activity and mental health occurred as a result of the COVID-19 pandemic.
There are many variables that can further contribute to the mental health status of college students during the pandemic, including their identity, family life, and background. We aimed to investigate the emotional, physical and social impacts on domestic US college students ages 18–24 and determine whether these impacts were significant among particular groups.
Recruitment and data collection
Two hundred (N = 200) domestic U.S. college students ages 18–24 attending a 4-year university in person before the COVID-19 pandemic were surveyed through Pollfish®. Pollfish® is a survey research platform that uses organic sampling built on Random Device Engagement (RDE). [ 9 ] Using artificial intelligence (AI) to track unique respondent identification, RDE reaches users in their natural environments as they participate in their daily activities through any device. [ 10 ] Pollfish®’s partnerships with over 120,000 applications and more than 700 million global users allow for random recruitment of participants fitting the specific inclusion criteria via in-app incentives specific to each user’s real-time activity on their respective devices [ 9 ]. The advanced AI technology and algorithm prevents fraud from single users on multiple accounts (SUMA) and suspicious or illogical responses to specific questions [ 10 ]. Pollfish® uses weighting to match the univariate distributions of age, gender, and geographic region. All results reported use this weighting.
Two screening questions were used to determine survey eligibility. These questions inquired whether participants are male or female aged 18–24 years, and whether they attended a domestic four-year U.S. college or university. The survey then consisted of 14 multiple choice questions. For some of the questions, multiple selections amongst the multiple choices were allowed, so that percentage totals could exceed 100%. The first 3 questions of the 14 inquired about background, including the participants’ year in college, whether they are the first in their family to attend college, and if they identify with the LGBTQIA+ community. The subsequent questions honed in on the physical, emotional, and social impacts of the COVID-19 pandemic. The final question was an open-ended one designed to capture the students’ verbatim feelings.
Statistical analysis
Data were analyzed using JMP Pro 14.1 for Windows [ 11 ]. Participants with a household income less than $50,000 annually were considered “low-income”. For comparing 2 × 2 contingency tables, Fisher’s two-tailed exact test was used. For comparing ordinal data, Wilcoxon’s rank-sum test was used. Ninety-five percent confidence intervals (CI) for odds ratios are Wald-based. All results used weighting generated by Pollfish® to match the univariate distributions of age and gender.
Ethics committee approval
This study (# 2020-966) was considered exempt by our institutional review board manager HCA Centralized Algorithms for Research Rules on IRB Exemptions (CARRIE).
A total of 200 people responded, of whom 50.6% were female (after adding weighting). Twenty three and 3/10% were first-year students, 39.9% were second-year students, 17.8% were third-year, 12.6% were fourth-year (seniors), and seven and one half percent were taking additional semesters (fifth or higher year). Fifty eight percent were first-generation students, and 36% considered themselves to be “a member of the LGBTQIA+ community.” The distributions of responses to each question are summarized in the Appendix, and each question is explored in detail in this section.
How has COVID-19 impacted your mental health?
For this question, multiple responses were allowed. Increased anxiety, depression, and feeling of loneliness were found in 60.8%, 54.1%, and 59.8% of the weighted population, respectively (Fig. 1 ). More than eighty percent (83.8%) reported an increase in at least one of these three symptoms. On the other hand, decreased anxiety, depression, and feelings of loneliness were respectively found in only 9.1%, 5.3%, and 4.6% of the population. For 10.7%, their mental health was unaffected. Using Fisher’s exact test, we found no significant differences in the prevalence of having at least one increased mental health symptom across first-generation status, gender, or LGBTQIA+ status. A general trend of decreased prevalence of symptoms as students drew closer to graduation was noticed. Using Fisher’s exact test, academic year and prevalence of mental health symptoms are not independent, with p < 0.0001.

Prevalence of mental health symptoms by academic year, and whether they increased
If you are not feeling at ease, what contributes MOST to your mental health status?
Twenty percent of respondents said that worries about the health of loved ones was their primary concern, 19.2% were most concerned about school/continuing education, 19.0% had anxiety about lack of proactivity, 15.9% were worried about finances, 10.8% were worried about future job offers, and 5.0% feared contracting the virus. Only 6.8% said that they were feeling at ease. Interestingly, there was no significant association between the proportion of respondents who were most worried about finances and income level (Fig. 2 ).

Causes of worry among students
Was it easier or harder to complete this semester away from campus?
Almost sixty-one percent of students found it harder to complete the semester away from campus, while 32.7% found it easier and 6.4% reported no change. There was no significant difference across age, gender, income level, LGBTQIA+ status, or first-generation status in this response.
How has COVID-19 affected your physical health?
Fifty percent of respondents indicated that they gained weight due to increased eating, while 20.2% reported that they felt/looked better due to exercise or dieting, 13.3% lost weight due to a lack of appetite, and 16.6% reported no changes. Among the students who reported an increased feeling of loneliness (59.8%), 57% reported that they gained weight, compared with just 39.4% of those who did not experience symptoms. Using Fisher’s exact test, this was significant with a p -value of 0.0301. The odds ratio (OR) is 2.04 (95% CI 1.15–3.62).
How has COVID-19 impacted your current and future plans?
COVID-19 disrupted the lives of most students, with only 26.4% stating the pandemic has not impacted their current or future plans. 27.1% lost an internship or job offer, 22.9% are taking a gap year or time off from school, and 31.8% need to support family. Only 16.6% say that the pandemic has given them other beneficial opportunities.
The groups of people most likely to have other beneficial opportunities due to the pandemic were men (OR 3.18, 95% CI 1.41–7.22, p = 0.0039), first-generation students (OR 2.27, 95% CI 0.99–5.19, p = 0.0329), and low-income students (OR 3.05, 95% CI 1.35–6.99, p = 0.0042). First-generation students were significantly more likely to take a gap year/time off from school (OR 2.42, 95% CI 1.17–5.02, p = 0.0251).
On the other hand, the groups that were significantly more likely to report no impact on future plans were women (OR 2.05, 95% CI 1.07–3.92, p = 0.0159), non-first-generation students (OR 3.12, 95% CI 1.62–5.97, p = 0.0003), and non-low-income students (OR 3.77, 95% CI 1.89–7.53, p < 0.0001). Given that these three groups correspond exactly to those which were least likely to say they gained beneficial opportunities, we investigated the rate at which gender, first-generation status, and low-income status affects having either a beneficial opportunity or no change in future plans. When performing this analysis, we found no significant differences across any of the three groups. Combined with the other evidence, this suggests that the key difference between demographic groups lies in the rate at which they gained beneficial opportunities in light of the pandemic.
How has COVID-19 impacted your relationships with your family?
29.4% of students had improved relationships with family, while 34.1% had strained relationships with family and 36.5% had no impact on relationships with family. The people who had strained relationships were significantly more likely to consider it harder to complete the semester at home (OR 2.59, 95% CI 1.36–4.94, p = 0.0036) compared to those who had improved relationships or no change.
How has COVID-19 impacted your relationships with your friends?
27.8% of students had improved relationships with friends, while 45.7% had strained relationships with friends and 26.5% had no impact on relationships with friends.
How have you specifically taken care of your mental health amidst COVID-19?
29.0% of students engaged in mindfulness activities (meditation, yoga, journaling, etc.). 46.7% were exercising or engaging in physical activity, 22.0% were using a health app, 17.7% were obtaining mental health care from a professional, and 30.3% were not taking any specific actions to take care of their mental health. Of the people who were exercising, 35.9% gained weight while 32.0% said they felt/looked better due to exercise or dieting. In contrast, of those who were not exercising, 62.2% gained weight and only 9.8% said they felt or looked better. Using Fisher’s exact test, this effect was significant with p < 0.0001.
At what point was your concern about COVID-19 heightened?
29.8% of students had their concern first heightened when college campuses sent students home, whereas 29.0% were first alarmed by states beginning lockdown guidelines. For 10.5%, they became more concerned when a friend or relative was diagnosed with COVID-19. For just 6.4%, the turning point was that friends or relatives were taking prevention measures seriously. Only 4.1% of the population indicated that they were not concerned about COVID-19. The distribution of responses was roughly equal across demographic groups.
How are you spending most of your time during the pandemic?
71.0% were watching TV shows or movies, 30.5% were reading books, 39.6% were exercising, 34.9% were learning new skills or picking up new hobbies, 33.6% were cooking or baking, 29.5% were working or interning, and 8.0% said they were not doing very much at all (Fig. 3 ). Note that the 39.6% figure of those exercising does not conflict with the 46.7% figure above, as some of the respondents may not be devoting very much time to exercise, and do not consider it a major use of their time during the pandemic.

How college students spent their time during the COVID-19 pandemic
Is there anything else you would like to share about the effect of COVID-19 on your mental health?
As this was a free-form text box, we used JMP’s text analysis suite to identify keywords. However, neither keyword identification nor singular value decomposition provided very much insight into the sentiments expressed. Given that this was an optional question, there was not enough information for numerical patterns to emerge. Instead, we have included a few quotes that demonstrate the range of ways that the COVID-19 pandemic has affected people’s mental health (not ordered by frequency).
“Everything has been so uncertain and has made me increasingly anxious”
“It is comforting to know that every college student in the country, and most around the world, are dealing with the same struggles that I am, and I am not alone in being fearful and anxious.”
“I smoke more”
“Its very hard to hold it together knowing the world as we once knew is no longer in existence..”
“Not getting help from my college financially has really drained me from even thinking about returning to college for FALL semester 2020.”
“One good thing is that it's given me more time to sleep, which has been one of the only benefits of the lockdown/pandemic.”
“It has increased productivity in approaching music & business”
The COVID-19 pandemic has brought severe educational and social repercussions, including the closure of college campuses as well as the introduction of online learning and social distancing at universities for the foreseeable future. College students were forced to abandon the social advantages of the so-called “college experience” (i.e. social gatherings, group studying, and in-person classes and meetings) to return home mid-semester. As reported by our survey, this triggered a decline in mental health measured by self-reported increased anxiety, depression, and loneliness. Consistent with these results, reports indicate that people of student status and ages 18–24 are at higher risk of anxiety and depression [ 12 ]. The stress associated with this abrupt social change, the disruptive factors that may exist at one’s home, and the fear of potentially contracting or spreading COVID-19 likely contributed to the development of trauma or stress-related disorders [ 13 ]. This accounts for the worsening mental health of domestic U.S. college students as shown by this survey, with significantly greater prevalence of symptoms among underclassmen that decreases with students closer to undergraduate completion. In line with the impacts we will discuss, this is likely due to the challenge of transitioning to college amidst a pandemic, the limited opportunities to form solid friendships, as well as a lack of human contact and in-person support.
Based on our survey’s results, the mental health status of the respondents has been most affected by their worries about the health of their loved ones amidst the COVID-19 pandemic. On top of that, many respondents feel uneasy about their plans for their continuing education, anxious about their lack of productivity at home, concerned about their finances and losing job and internship prospects, and worried about contracting the virus. These factors likely made it harder for students to complete the Spring 2020 semester at home, as many respondents have indicated. Indeed, most respondents indicated that their concern about the ongoing pandemic largely began when college campuses began to shut down or when states issued lockdown guidelines shortly after. These events evidently served as a turning point in the mental health of the respondents. As the pandemic ensued, the respondents reported that their lives were disrupted in significant ways. For instance, many reported to have lost an internship or job offer. Others reported the need to take a gap year. In addition, many respondents indicated that they now have the added responsibility of supporting their family in some way. Of the respondents who claimed that the COVID-19 pandemic strained family relationships, most admitted that it has been harder to work from home than at school. These results are summarized in Fig. 4 .

Ways in which COVID-19 has affected the mental health of college students
More than one third of first-generation students experienced increased anxiety and a quarter found it harder to complete the semester at home. Accordingly, significantly more first-generation students reported taking a gap year or time off from school. First generation students were more likely able to take advantage of opportunities due to the pandemic, indicating access to support systems that may have allowed these students to take time off from school in the first place. Men and low-income students were also more likely to benefit from opportunities due to the pandemic while women, non first-generation, and non low-income students were more likely to report no impacts. However, there were no significant differences across these three demographic statuses, indicating that the main differences were solely in whether or not they gained beneficial opportunities due to the pandemic. Taken together, it appears that first generation and low-income students likely sought out more support during the pandemic, which has helped them overcome pre-pandemic anxiety regarding communicating with campus faculty and staff and utilizing support services [ 14 ]. In regards to male students who benefitted from these opportunities, they likely took time off from school as the number of men who have enrolled in college this Fall 2020 declined by seven times compared to the number of women enrolled [ 15 ], potentially due to the increased mental health issues experienced by all. The key difference is that men are less likely to seek help for mental health difficulties compared to women even pre-pandemic [ 16 ].
On the other hand, there were mixed experiences (albeit statistically insignificant) for LGBTQIA+ students with regard to anxiety, with a quarter reported increased levels and a similar number reporting decreased levels of anxiety. There were similarly mixed experiences in completing the semester from home. This may be due to LGBTQIA+ students accessing necessary resources as sixty-two percent of U.S. colleges and universities have LGBTQIA+ support groups [ 17 ] that likely serve as a valuable resource for these students throughout the pandemic.
Presumably due to increased stress factors at home and distance barriers, most respondents indicated that the COVID-19 pandemic strained relationships with their friends. While communications with friends declined, most respondents reported to be spending most of their free time watching TV because of widespread state and local lockdown orders. According to a health survey in England from 2012, watching TV for two hours or more on a daily basis is associated with mental health disorders, measured by a poor performance on the General Health Questionnaire and Warwick-Edinburgh Mental Well-being Scale [ 18 ]. On the other hand, nearly 40% of respondents indicated that they spent time exercising. Physical exercise has been proven to alleviate anxiety and depression, while increasing one’s mood and cognitive function [ 19 ]. Roughly half of the respondents claimed that they used exercise to take care of their mental health. Of those people, most reported feeling better. However, over 30% of respondents admitted to not specifically taking care of their mental health. Most people reported that they gained weight, particularly those who reported increased loneliness. The isolation and lack of contact may have led affected students to seek comfort food or decrease their daily activity levels, whether it may be training on a sports team or walking to classes and other commitments.
Similar to our findings that the COVID-19 pandemic has led to an overall reduction in the mental health of US college students, a study in China reported that about 40% of female adolescents have suffered from depression. The study cited distance learning, concern about the pandemic, and a decrease in physical exercise and sleep as independent factors causing this increase in depression [ 20 ]. Undoubtedly, the pandemic has caused many to experience feelings of loneliness and isolation. Furthermore, it has caused many individuals’ pre-existing mental health conditions to deteriorate without access to the appropriate services [ 21 ].
These services are offered on most college campuses but are more difficult to access in the world of online learning. According to a study in the New York City metropolitan area, only about half of the surveyed colleges offered information about remote counseling on their website and less than 60% of college counseling websites even offered directions for students experiencing a mental health emergency [ 22 ]. Furthermore, many news outlets report that out-of-state students have been unable to receive mental health services from their schools due to state-dependent licensures—some of which require psychologists to apply for a temporary license or receive special permission to practice [ 23 ]. Although some policies have been relaxed, students still face geographic, time, and financial barriers to access these necessary mental health services [ 23 , 24 , 25 ]. Additionally, the flexibility extended for telemedicine providers due to the pandemic being a public health emergency began to expire in Fall 2020, and navigating these policies is time-consuming and confusing for healthcare providers [ 25 ]. All of these obstacles have contributed to out-of-state students losing their mental health support completely in the face of the clear decline in mental health we have found, as supported by recent similar studies [ 26 , 27 , 28 , 29 ].
To combat the mental health challenges experienced by many US college students amidst the COVID-19 pandemic, colleges and universities across the country could take steps to expand access to virtual mental health resources and professional guidance. Some institutions have taken to a 24/7 crisis support line as well as virtual resources and emergency funding provided by the CARES Act distributed through the Higher Education Emergency Relief Fund [ 30 ]. Some universities were able to refund costs from room and board, which likely contributed to easing financial distress [ 31 ]. At the federal level, the PSYPACT agreement was passed—allowing interstate practice within the fourteen states it has been enacted in [ 32 ]ーand the TREAT Act that would allow healthcare professionals to render services anywhere during the COVID-19 pandemic was proposed but has yet to be implemented [ 33 ].
Limitations
The survey results are limited by the fact that only students who are registered with Pollfish® as publishers have the opportunity to participate in this survey. Potentially due to the monetary incentive given by Pollfish® to the respondents of their surveys, first generation and low income students are slightly overrepresented. In this survey, 61.0% of students are first generation, 35.5% being low income which is higher than the national average of 56.0% first generation students [ 34 ]. However, a study by Haenz et al. at the University of California, Los Angeles reports that roughly 50.0% of first generation students are low-income [ 35 ], which may be accounted for by the additional 10.5% of students who preferred not to reveal their income status in our study. Additionally, there are more students who identify as a member of the LGBTQIA+ community (36.5%) compared to the national average of 18.2% [ 36 ]. Our slightly disproportionate sample indicates that our findings may not be fully representative of all U.S. college students.
Future avenues of investigation include looking into specific experiences of these groups as well as other factors, such as the experiences of international students, of associate degree program students, community college students, or students completing online degrees and areas of improvement for the specific support systems in place at these educational institutions for these students since the pandemic.
The outbreak of COVID-19 has taken a universal toll on almost all aspects of life. As cases rapidly increased with great incidence, dense areas and indoor public spaces were closed and physical distancing as well as other preventative measures were enforced. These safety measures led to abrupt closures of schools and educational institutions, and a rushed transition to remote learning. Many reported worries for the health of loved ones most impacted their mental health, and the need to take care of family most affected current and future plans. Given that most students’ concerns were heightened when college campuses sent students home as well as the detrimental effects of the COVID-19 pandemic on students’ mental health, it is crucial for colleges as well as federal regulations to provide the appropriate accommodations and access to mental health care to ensure well-being and safety are prioritized as much asーif not more thanーeducation.
Availability of the data and materials
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.
Abbreviations
Confidence interval
2019 Novel Coronavirus
Lesbian, gay, bisexual, transgender, queer or questioning, intersex, and asexual or allied
Lesbian, Gay, Bisexual, Transgender, Queer, Intersex, Agender, Asexual and other queer-identifying community
Psychology Interjurisdictional Compact, an interstate compact facilitated by the Association of State and Provincial Psychology Boards (ASPPB)
Coronavirus Aid, Relief, and Economic Security Act, S.3548 bill introduced in 19 March 2020 by Senator McConnell
Temporary Reciprocity to Ensure Access to Treatment Act, S.4421 bill introduced in 04 August 2020 by Senator Murphy
Zhai P, Ding Y, Wu X et al. The epidemiology, diagnosis, and treatment of COVID-19. Int J Antimicrob Agents. 2020;55:5. https://doi.org/10.1016/j.ijantimicag.2020.105955
Wang Y, Wang Y, Chen Y, et al. Unique epidemiological and clinical features of the emerging 2019 novel coronavirus pneumonia (COVID-19) implicate special control measures. J Med Virol. 2020;92(6):568–76. https://doi.org/10.1002/jmv.25748 .
Article PubMed Google Scholar
Huckins JF, DaSilva AW, Wang W, Hedlund E, Rogers C, Nepal SK, Wu J, Obuchi M, Murphy EI, Meyer ML, Wagner DD, Holtzheimer PE, Campbell AT. Mental Health and behavior of college students during the early phases of the COVID-19 pandemic: longitudinal smartphone and ecological momentary assessment study. J Med Internet Res. 2020;22:6. https://doi.org/10.2196/20185 .
Salerno JP, Williams ND, Gattamorta KA. LGBTQ populations: psychologically vulnerable communities in the COVID-19 pandemic. Psychol Trauma Theory Res Pract Policy. 2020;12(1):239–42. https://doi.org/10.1037/tra0000837 .
Article Google Scholar
Azar KMJ, Shen, Z., Romanelli RJ. Disparities in outcomes among COVID-19 patients in a large health care system in California. Health Aff. 2020;39:7. https://doi.org/10.1377/hlthaff.2020.00598
Verma K. The mental health impact of the COVID-19 epidemic on college students in India. Asian J Psychiatr. 2020;53. https://doi.org/10.1016/j.ajp.2020.102398 ( Epub 2020 Aug 31 ).
Kleiman EM, Yeager AL, Grove JL, Kellerman JK, Kim JS. Real-time mental health impact of the COVID-19 pandemic on college students: ecological momentary assessment study. JMIR Ment Health. 2020;7:12. https://doi.org/10.2196/24815 .
Ryerson NC, Wilson OWA, Pena A, Duffy M, Bopp M. What happens when the party moves home? The effect of the COVID-19 pandemic on U.S. college student alcohol consumption as a function of legal drinking status using longitudinal data. Transl Behav Med. 2021;11(3):772–774. https://doi.org/10.1093/tbm/ibab006 .
What Is Organic Probability Sampling? | Survey Methodology. 2020. https://www.pollfish.com/methodology . Accessed 6 June 2021.
Rothschild D, Konitzer T. Random Device Engagement (RDE) With Organic Samples . New York: Pollfish® Inc; 2020. https://resources.pollfish.com/market-research/random-device-engagement-and-organic-sampling . Accessed 6 June 2021.
JMP Pro®, Version 14.1. SAS Institute Inc., Cary, NC, 1989–2020.
Solomou I, Constantinidou F. Prevalence and predictors of anxiety and depression symptoms during the COVID-19 pandemic and compliance with precautionary measures: age and sex matter. Int J Environ Res Public Health. 2020;17(14):E4924. https://doi.org/10.3390/ijerph17144924 .
Esterwood E, Saeed SA. Past epidemics, natural disasters, COVID19, and mental health: learning from history as we deal with the present and prepare for the future. Psychiatr Q. 2020;1–13. https://doi.org/10.1007/s11126-020-09808-4
The Pell Institute for the Study of Opportunity in Higher Education. Moving Beyond Access College Success For Low-Income, First-Generation Students [Internet]. Washington, DC: The Pell Institute for the Study of Opportunity in Higher Education; 2008. https://files.eric.ed.gov/fulltext/ED504448.pdf
National Student Clearinghouse Research Center. Term Enrollment Estimates Fall 2020 [Internet]. Herndon, VA: National Student Clearinghouse; 2020. Available from: https://nscresearchcenter.org/wp-content/uploads/CTEE_Report_Fall_2020.pdf
Sagar-Ouriaghli I, Godfrey E, Bridge L, et al. Improving mental health service utilization among men: a systematic review and synthesis of behavior change techniques within interventions targeting help-seeking. Am. J. Men's Health. 2019;13:3. https://doi.org/10.1177/1557988319857009
Coley J, Das D. Creating safe spaces: opportunities, resources, and LGBTQ student groups at U.S. Colleges and Universities. Socius: Sociological Research for a Dynamic World. 2020;6. https://doi.org/10.1177/2378023120971472
Shiue I. Modeling indoor TV/screen viewing and adult physical and mental health: Health Survey for England, 2012. Environ Sci Pollut Res Int. 2016;23(12):11708–15. https://doi.org/10.1007/s11356-016-6354-5 .
Article PubMed PubMed Central Google Scholar
Sharma A, Madaan V, Petty FD. Exercise for mental health. Prim Care Companion J Clin Psychiatry. 2006;8(2):106. https://doi.org/10.4088/pcc.v08n0208a .
Zhou J, Yuan X, Qi H, et al. Prevalence of depression and its correlative factors among female adolescents in China during the coronavirus disease 2019 outbreak. Global Health. 2020;16(1):69. https://doi.org/10.1186/s12992-020-00601-3 .
Sheridan Rains L, Johnson S, Barnett P, et al. Early impacts of the COVID-19 pandemic on mental health care and on people with mental health conditions: framework synthesis of international experiences and responses. Soc Psychiatry Psychiatr Epidemiol. 2020;1–12. https://doi.org/10.1007/s00127-020-01924-7
Seidel EJ, Mohlman J, Basch CH, Fera J, Cosgrove A, Ethan D. Communicating mental health support to college students during COVID-19: an exploration of website messaging. J Community Health. 2020;1–4. https://doi.org/10.1007/s10900-020-00905-w
The Washington Post. College students count on their schools for mental-health help, but now many can’t get it. https://www.washingtonpost.com/local/education/college-students-count-on-their-schools-for-mental-health-help-but-now-many-cant-get-it/2020/05/28/e6f6e710-8b2b-11ea-ac8a-fe9b8088e101_story.html . Published 2020. Accessed March 1, 2021
Choy Y. Filling Telehealth Gaps in College Mental Health. Psychiatric Times . 2020. https://www.psychiatrictimes.com/view/filling-telehealth-gaps-college-mental-health . Accessed March 1, 2021.
Gulino, E. COVID-19 Took Away My On-Campus Education — & My Therapist With It. Refinery29 . 2020. https://www.refinery29.com/en-us/2020/09/10027717/college-mental-health-services-covid . Accessed March 1, 2021.
Sahu P. Closure of universities due to coronavirus disease 2019 (COVID-19): impact on education and mental health of students and academic staff. Cureus. 2020 Apr;12(4). https://doi.org/10.7759/cureus.7541
Son C, Hegde S, Smith A, et al. Effects of COVID-19 on college students’ mental health in the United States: Interview survey study. J Med Internet Res. 2020;22(9). https://doi.org/10.2196/21279 .
Kecojevic A, Basch C, Sullivan M, et al. The impact of the COVID-19 epidemic on mental health of undergraduate students in New Jersey, cross-sectional study. PLOS ONE. 2020;15(9). https://doi.org/10.1371/journal.pone.0239696
Wang X, Hegde S, Son C, et al. Investigating Mental Health of US College Students During the COVID-19 Pandemic: Cross-Sectional Survey Study. Journal of Medical Internet Research. 2020;22(9). https://doi.org/10.2196/22817
CARES Act: Higher Education Emergency Relief Fund. https://www2.ed.gov/about/offices/list/ope/caresact.html (2021). Accessed March 1, 2021.
Zhai Y, Du X (2020) Addressing collegiate mental health amid COVID-19 pandemic. Psychiatry Research. 288:113003.
Clay R. CMS recognizes PSYPACT licensure requirements for interstate practice. American Psychological Association Services, Inc. 2020. https://www.apaservices.org/practice/legal/technology/psypact-licensure-requirements?_ga=2.71722714.834013392.1600809295-1830711977.1599002157 . Accessed March 1, 2021.
Murphy, Blunt Introduce Legislation to Allow Health Care Professionals to Render Services Anywhere throughout Covid-19 Pandemic. U.S. Senator Chris Murphy of Connecticut. 2020. https://www.murphy.senate.gov/newsroom/press-releases/murphy-blunt-introduce-legislation-to-allow-health-care-professionals-to-render-services-anywhere-throughout-covid-19-pandemic -. Accessed 01 March 2021.
RTI International. First-generation College Students: Demographic Characteristics and Postsecondary Enrollment . NASPA, Washington, DC. 2019. https://firstgen.naspa.org/files/dmfile/FactSheet-01.pdf . Accessed 01 March 2021.
First In My Family: A Profile Of First-Generation College Students At Four-Year Institutions Since 1971 . University of California, Los Angeles; The Foundation for Independent Higher Education; Los Angeles, CA. 2007. https://www.heri.ucla.edu/PDFs/pubs/TFS/Special/Monographs/FirstInMyFamily.pdf . Accessed 01 March 2021.
American College Health Association- National College Health Assessment. American College Health Association-National College Health Assessment II: Undergraduate Student Reference Group Executive Summary. American College Health Association; Hanover, MD. 2016. https://www.acha.org/documents/ncha/NCHA-II_FALL_2016_UNDERGRADUATE_REFERENCE_GROUP_EXECUTIVE_SUMMARY.pdf . Accessed 01 March 2021.
Download references
Acknowledgements
This research was supported (in whole or in part) by HCA Healthcare and/or an HCA Healthcare affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.
No funding was received for this study.
Author information
Authors and affiliations.
Brown University, Providence, RI, USA
Jenny Lee, Matthew Solomon, Tej Stead & Bryan Kwon
Envision Physician Services, Plantation, FL, USA
Latha Ganti
Departments of Emergency Medicine and Neurology, University of Central Florida, 6950 Lake Nona Blvd, Orlando, FL, 32832, USA
Ocala Regional Medical Center, Ocala, FL, USA
You can also search for this author in PubMed Google Scholar
Contributions
The survey was designed by JL, MS, TS and BK. MS managed data capture. TS performed the statistical analysis. JL designed the infographic. LG supervised the conduct of the research. All authors read and approved the final manuscript.
Corresponding author
Correspondence to Latha Ganti .
Ethics declarations
Ethics approval and consent to participate.
This study was submitted to our institutional ethics committee, the HCA Centralized Algorithms for Research Rules on IRB Exemptions (CARRIE)/IRB manager. The study was issued ID# 2020–966, and was considered exempt from IRB oversight per 45CFR46.102(l) and 45CFR46.104.
Consent for publication
Not applicable as no identifying information/images are present in the study.
Competing interests
The authors declare they have no competing interests.
Additional information
Publisher's note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
. Appendix listing survey questions.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Lee, J., Solomon, M., Stead, T. et al. Impact of COVID-19 on the mental health of US college students. BMC Psychol 9 , 95 (2021). https://doi.org/10.1186/s40359-021-00598-3
Download citation
Received : 13 December 2020
Accepted : 24 May 2021
Published : 08 June 2021
DOI : https://doi.org/10.1186/s40359-021-00598-3
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Mental health
BMC Psychology
ISSN: 2050-7283
- General enquiries: [email protected]
Resources for
- Prospective Students
- Current Students
- Admin Resources
Search form
Essays reveal experiences during pandemic, unrest.

Field study students share their thoughts
Members of Advanced Field Study, a select group of Social Ecology students who are chosen from a pool of applicants to participate in a year-long field study experience and course, had their internships and traditional college experience cut short this year. During our final quarter of the year together, during which we met weekly for two hours via Zoom, we discussed their reactions as the world fell apart around them. First came the pandemic and social distancing, then came the death of George Floyd and the response of the Black Lives Matter movement, both of which were imprinted on the lives of these students. This year was anything but dull, instead full of raw emotion and painful realizations of the fragility of the human condition and the extent to which we need one another. This seemed like the perfect opportunity for our students to chronicle their experiences — the good and the bad, the lessons learned, and ways in which they were forever changed by the events of the past four months. I invited all of my students to write an essay describing the ways in which these times had impacted their learning and their lives during or after their time at UCI. These are their voices. — Jessica Borelli , associate professor of psychological science
Becoming Socially Distant Through Technology: The Tech Contagion

The current state of affairs put the world on pause, but this pause gave me time to reflect on troubling matters. Time that so many others like me probably also desperately needed to heal without even knowing it. Sometimes it takes one’s world falling apart for the most beautiful mosaic to be built up from the broken pieces of wreckage.
As the school year was coming to a close and summer was edging around the corner, I began reflecting on how people will spend their summer breaks if the country remains in its current state throughout the sunny season. Aside from living in the sunny beach state of California where people love their vitamin D and social festivities, I think some of the most damaging effects Covid-19 will have on us all has more to do with social distancing policies than with any inconveniences we now face due to the added precautions, despite how devastating it may feel that Disneyland is closed to all the local annual passholders or that the beaches may not be filled with sun-kissed California girls this summer. During this unprecedented time, I don’t think we should allow the rare opportunity we now have to be able to watch in real time how the effects of social distancing can impact our mental health. Before the pandemic, many of us were already engaging in a form of social distancing. Perhaps not the exact same way we are now practicing, but the technology that we have developed over recent years has led to a dramatic decline in our social contact and skills in general.
The debate over whether we should remain quarantined during this time is not an argument I am trying to pursue. Instead, I am trying to encourage us to view this event as a unique time to study how social distancing can affect people’s mental health over a long period of time and with dramatic results due to the magnitude of the current issue. Although Covid-19 is new and unfamiliar to everyone, the isolation and separation we now face is not. For many, this type of behavior has already been a lifestyle choice for a long time. However, the current situation we all now face has allowed us to gain a more personal insight on how that experience feels due to the current circumstances. Mental illness continues to remain a prevalent problem throughout the world and for that reason could be considered a pandemic of a sort in and of itself long before the Covid-19 outbreak.
One parallel that can be made between our current restrictions and mental illness reminds me in particular of hikikomori culture. Hikikomori is a phenomenon that originated in Japan but that has since spread internationally, now prevalent in many parts of the world, including the United States. Hikikomori is not a mental disorder but rather can appear as a symptom of a disorder. People engaging in hikikomori remain confined in their houses and often their rooms for an extended period of time, often over the course of many years. This action of voluntary confinement is an extreme form of withdrawal from society and self-isolation. Hikikomori affects a large percent of people in Japan yearly and the problem continues to become more widespread with increasing occurrences being reported around the world each year. While we know this problem has continued to increase, the exact number of people practicing hikikomori is unknown because there is a large amount of stigma surrounding the phenomenon that inhibits people from seeking help. This phenomenon cannot be written off as culturally defined because it is spreading to many parts of the world. With the technology we now have, and mental health issues on the rise and expected to increase even more so after feeling the effects of the current pandemic, I think we will definitely see a rise in the number of people engaging in this social isolation, especially with the increase in legitimate fears we now face that appear to justify the previously considered irrational fears many have associated with social gatherings. We now have the perfect sample of people to provide answers about how this form of isolation can affect people over time.
Likewise, with the advancements we have made to technology not only is it now possible to survive without ever leaving the confines of your own home, but it also makes it possible for us to “fulfill” many of our social interaction needs. It’s very unfortunate, but in addition to the success we have gained through our advancements we have also experienced a great loss. With new technology, I am afraid that we no longer engage with others the way we once did. Although some may say the advancements are for the best, I wonder, at what cost? It is now commonplace to see a phone on the table during a business meeting or first date. Even worse is how many will feel inclined to check their phone during important or meaningful interactions they are having with people face to face. While our technology has become smarter, we have become dumber when it comes to social etiquette. As we all now constantly carry a mini computer with us everywhere we go, we have in essence replaced our best friends. We push others away subconsciously as we reach for our phones during conversations. We no longer remember phone numbers because we have them all saved in our phones. We find comfort in looking down at our phones during those moments of free time we have in public places before our meetings begin. These same moments were once the perfect time to make friends, filled with interactive banter. We now prefer to stare at other people on our phones for hours on end, and often live a sedentary lifestyle instead of going out and interacting with others ourselves.
These are just a few among many issues the advances to technology led to long ago. We have forgotten how to practice proper tech-etiquette and we have been inadvertently practicing social distancing long before it was ever required. Now is a perfect time for us to look at the society we have become and how we incurred a different kind of pandemic long before the one we currently face. With time, as the social distancing regulations begin to lift, people may possibly begin to appreciate life and connecting with others more than they did before as a result of the unique experience we have shared in together while apart.
Maybe the world needed a time-out to remember how to appreciate what it had but forgot to experience. Life is to be lived through experience, not to be used as a pastime to observe and compare oneself with others. I’ll leave you with a simple reminder: never forget to take care and love more because in a world where life is often unpredictable and ever changing, one cannot risk taking time or loved ones for granted. With that, I bid you farewell, fellow comrades, like all else, this too shall pass, now go live your best life!
Privilege in a Pandemic

Covid-19 has impacted millions of Americans who have been out of work for weeks, thus creating a financial burden. Without a job and the certainty of knowing when one will return to work, paying rent and utilities has been a problem for many. With unemployment on the rise, relying on unemployment benefits has become a necessity for millions of people. According to the Washington Post , unemployment rose to 14.7% in April which is considered to be the worst since the Great Depression.
Those who are not worried about the financial aspect or the thought never crossed their minds have privilege. Merriam Webster defines privilege as “a right or immunity granted as a peculiar benefit, advantage, or favor.” Privilege can have a negative connotation. What you choose to do with your privilege is what matters. Talking about privilege can bring discomfort, but the discomfort it brings can also carry the benefit of drawing awareness to one’s privilege, which can lead the person to take steps to help others.
I am a first-generation college student who recently transferred to a four-year university. When schools began to close, and students had to leave their on-campus housing, many lost their jobs.I was able to stay on campus because I live in an apartment. I am fortunate to still have a job, although the hours are minimal. My parents help pay for school expenses, including housing, tuition, and food. I do not have to worry about paying rent or how to pay for food because my parents are financially stable to help me. However, there are millions of college students who are not financially stable or do not have the support system I have. Here, I have the privilege and, thus, I am the one who can offer help to others. I may not have millions in funding, but volunteering for centers who need help is where I am able to help. Those who live in California can volunteer through Californians For All or at food banks, shelter facilities, making calls to seniors, etc.
I was not aware of my privilege during these times until I started reading more articles about how millions of people cannot afford to pay their rent, and landlords are starting to send notices of violations. Rather than feel guilty and be passive about it, I chose to put my privilege into a sense of purpose: Donating to nonprofits helping those affected by COVID-19, continuing to support local businesses, and supporting businesses who are donating profits to those affected by COVID-19.
My World is Burning

As I write this, my friends are double checking our medical supplies and making plans to buy water and snacks to pass out at the next protest we are attending. We write down the number for the local bailout fund on our arms and pray that we’re lucky enough not to have to use it should things get ugly. We are part of a pivotal event, the kind of movement that will forever have a place in history. Yet, during this revolution, I have papers to write and grades to worry about, as I’m in the midst of finals.
My professors have offered empty platitudes. They condemn the violence and acknowledge the stress and pain that so many of us are feeling, especially the additional weight that this carries for students of color. I appreciate their show of solidarity, but it feels meaningless when it is accompanied by requests to complete research reports and finalize presentations. Our world is on fire. Literally. On my social media feeds, I scroll through image after image of burning buildings and police cars in flames. How can I be asked to focus on school when my community is under siege? When police are continuing to murder black people, adding additional names to the ever growing list of their victims. Breonna Taylor. Ahmaud Arbery. George Floyd. David Mcatee. And, now, Rayshard Brooks.
It already felt like the world was being asked of us when the pandemic started and classes continued. High academic expectations were maintained even when students now faced the challenges of being locked down, often trapped in small spaces with family or roommates. Now we are faced with another public health crisis in the form of police violence and once again it seems like educational faculty are turning a blind eye to the impact that this has on the students. I cannot study for exams when I am busy brushing up on my basic first-aid training, taking notes on the best techniques to stop heavy bleeding and treat chemical burns because at the end of the day, if these protests turn south, I will be entering a warzone. Even when things remain peaceful, there is an ugliness that bubbles just below the surface. When beginning the trek home, I have had armed members of the National Guard follow me and my friends. While kneeling in silence, I have watched police officers cock their weapons and laugh, pointing out targets in the crowd. I have been emailing my professors asking for extensions, trying to explain that if something is turned in late, it could be the result of me being detained or injured. I don’t want to be penalized for trying to do what I wholeheartedly believe is right.
I have spent my life studying and will continue to study these institutions that have been so instrumental in the oppression and marginalization of black and indigenous communities. Yet, now that I have the opportunity to be on the frontlines actively fighting for the change our country so desperately needs, I feel that this study is more of a hindrance than a help to the cause. Writing papers and reading books can only take me so far and I implore that professors everywhere recognize that requesting their students split their time and energy between finals and justice is an impossible ask.
Opportunity to Serve

Since the start of the most drastic change of our lives, I have had the privilege of helping feed more than 200 different families in the Santa Ana area and even some neighboring cities. It has been an immense pleasure seeing the sheer joy and happiness of families as they come to pick up their box of food from our site, as well as a $50 gift card to Northgate, a grocery store in Santa Ana. Along with donating food and helping feed families, the team at the office, including myself, have dedicated this time to offering psychosocial and mental health check-ups for the families we serve.
Every day I go into the office I start my day by gathering files of our families we served between the months of January, February, and March and calling them to check on how they are doing financially, mentally, and how they have been affected by COVID-19. As a side project, I have been putting together Excel spreadsheets of all these families’ struggles and finding a way to turn their situation into a success story to share with our board at PY-OCBF and to the community partners who make all of our efforts possible. One of the things that has really touched me while working with these families is how much of an impact this nonprofit organization truly has on family’s lives. I have spoken with many families who I just call to check up on and it turns into an hour call sharing about how much of a change they have seen in their child who went through our program. Further, they go on to discuss that because of our program, their children have a different perspective on the drugs they were using before and the group of friends they were hanging out with. Of course, the situation is different right now as everyone is being told to stay at home; however, there are those handful of kids who still go out without asking for permission, increasing the likelihood they might contract this disease and pass it to the rest of the family. We are working diligently to provide support for these parents and offering advice to talk to their kids in order to have a serious conversation with their kids so that they feel heard and validated.
Although the novel Coronavirus has impacted the lives of millions of people not just on a national level, but on a global level, I feel that in my current position, it has opened doors for me that would have otherwise not presented themselves. Fortunately, I have been offered a full-time position at the Project Youth Orange County Bar Foundation post-graduation that I have committed to already. This invitation came to me because the organization received a huge grant for COVID-19 relief to offer to their staff and since I was already part-time, they thought I would be a good fit to join the team once mid-June comes around. I was very excited and pleased to be recognized for the work I have done at the office in front of all staff. I am immensely grateful for this opportunity. I will work even harder to provide for the community and to continue changing the lives of adolescents, who have steered off the path of success. I will use my time as a full-time employee to polish my resume, not forgetting that the main purpose of my moving to Irvine was to become a scholar and continue the education that my parents couldn’t attain. I will still be looking for ways to get internships with other fields within criminology. One specific interest that I have had since being an intern and a part-time employee in this organization is the work of the Orange County Coroner’s Office. I don’t exactly know what enticed me to find it appealing as many would say that it is an awful job in nature since it relates to death and seeing people in their worst state possible. However, I feel that the only way for me to truly know if I want to pursue such a career in forensic science will be to just dive into it and see where it takes me.
I can, without a doubt, say that the Coronavirus has impacted me in a way unlike many others, and for that I am extremely grateful. As I continue working, I can also state that many people are becoming more and more hopeful as time progresses. With people now beginning to say Stage Two of this stay-at-home order is about to allow retailers and other companies to begin doing curbside delivery, many families can now see some light at the end of the tunnel.
Let’s Do Better

This time of the year is meant to be a time of celebration; however, it has been difficult to feel proud or excited for many of us when it has become a time of collective mourning and sorrow, especially for the Black community. There has been an endless amount of pain, rage, and helplessness that has been felt throughout our nation because of the growing list of Black lives we have lost to violence and brutality.
To honor the lives that we have lost, George Floyd, Tony McDade, Breonna Taylor, Ahmaud Arbery, Eric Garner, Oscar Grant, Michael Brown, Trayon Martin, and all of the other Black lives that have been taken away, may they Rest in Power.
Throughout my college experience, I have become more exposed to the various identities and the upbringings of others, which led to my own self-reflection on my own privileged and marginalized identities. I identify as Colombian, German, and Mexican; however navigating life as a mixed race, I have never been able to identify or have one culture more salient than the other. I am visibly white-passing and do not hold any strong ties with any of my ethnic identities, which used to bring me feelings of guilt and frustration, for I would question whether or not I could be an advocate for certain communities, and whether or not I could claim the identity of a woman of color. In the process of understanding my positionality, I began to wonder what space I belonged in, where I could speak up, and where I should take a step back for others to speak. I found myself in a constant theme of questioning what is my narrative and slowly began to realize that I could not base it off lone identities and that I have had the privilege to move through life without my identities defining who I am. Those initial feelings of guilt and confusion transformed into growth, acceptance, and empowerment.
This journey has driven me to educate myself more about the social inequalities and injustices that people face and to focus on what I can do for those around me. It has motivated me to be more culturally responsive and competent, so that I am able to best advocate for those around me. Through the various roles I have worked in, I have been able to listen to a variety of communities’ narratives and experiences, which has allowed me to extend my empathy to these communities while also pushing me to continue educating myself on how I can best serve and empower them. By immersing myself amongst different communities, I have been given the honor of hearing others’ stories and experiences, which has inspired me to commit myself to support and empower others.
I share my story of navigating through my privileged and marginalized identities in hopes that it encourages others to explore their own identities. This journey is not an easy one, and it is an ongoing learning process that will come with various mistakes. I have learned that with facing our privileges comes feelings of guilt, discomfort, and at times, complacency. It is very easy to become ignorant when we are not affected by different issues, but I challenge those who read this to embrace the discomfort. With these emotions, I have found it important to reflect on the source of discomfort and guilt, for although they are a part of the process, in taking the steps to become more aware of the systemic inequalities around us, understanding the source of discomfort can better inform us on how we perpetuate these systemic inequalities. If we choose to embrace ignorance, we refuse to acknowledge the systems that impact marginalized communities and refuse to honestly and openly hear cries for help. If we choose our own comfort over the lives of those being affected every day, we can never truly honor, serve, or support these communities.
I challenge any non-Black person, including myself, to stop remaining complacent when injustices are committed. We need to consistently recognize and acknowledge how the Black community is disproportionately affected in every injustice experienced and call out anti-Blackness in every role, community, and space we share. We need to keep ourselves and others accountable when we make mistakes or fall back into patterns of complacency or ignorance. We need to continue educating ourselves instead of relying on the emotional labor of the Black community to continuously educate us on the history of their oppressions. We need to collectively uplift and empower one another to heal and rise against injustice. We need to remember that allyship ends when action ends.
To the Black community, you are strong. You deserve to be here. The recent events are emotionally, mentally, and physically exhausting, and the need for rest to take care of your mental, physical, and emotional well-being are at an all time high. If you are able, take the time to regain your energy, feel every emotion, and remind yourself of the power you have inside of you. You are not alone.
The Virus That Makes You Forget

Following Jan. 1 of 2020 many of my classmates and I continued to like, share, and forward the same meme. The meme included any image but held the same phrase: I can see 2020. For many of us, 2020 was a beacon of hope. For the Class of 2020, this meant walking on stage in front of our families. Graduation meant becoming an adult, finding a job, or going to graduate school. No matter what we were doing in our post-grad life, we were the new rising stars ready to take on the world with a positive outlook no matter what the future held. We felt that we had a deal with the universe that we were about to be noticed for our hard work, our hardships, and our perseverance.
Then March 17 of 2020 came to pass with California Gov. Newman ordering us to stay at home, which we all did. However, little did we all know that the world we once had open to us would only be forgotten when we closed our front doors.
Life became immediately uncertain and for many of us, that meant graduation and our post-graduation plans including housing, careers, education, food, and basic standards of living were revoked! We became the forgotten — a place from which many of us had attempted to rise by attending university. The goals that we were told we could set and the plans that we were allowed to make — these were crushed before our eyes.
Eighty days before graduation, in the first several weeks of quarantine, I fell extremely ill; both unfortunately and luckily, I was isolated. All of my roommates had moved out of the student apartments leaving me with limited resources, unable to go to the stores to pick up medicine or food, and with insufficient health coverage to afford a doctor until my throat was too swollen to drink water. For nearly three weeks, I was stuck in bed, I was unable to apply to job deadlines, reach out to family, and have contact with the outside world. I was forgotten.
Forty-five days before graduation, I had clawed my way out of illness and was catching up on an honors thesis about media depictions of sexual exploitation within the American political system, when I was relayed the news that democratic presidential candidate Joe Biden was accused of sexual assault. However, when reporting this news to close friends who had been devastated and upset by similar claims against past politicians, they all were too tired and numb from the quarantine to care. Just as I had written hours before reading the initial story, history was repeating, and it was not only I who COVID-19 had forgotten, but now survivors of violence.
After this revelation, I realize the silencing factor that COVID-19 has. Not only does it have the power to terminate the voices of our older generations, but it has the power to silence and make us forget the voices of every generation. Maybe this is why social media usage has gone up, why we see people creating new social media accounts, posting more, attempting to reach out to long lost friends. We do not want to be silenced, moreover, we cannot be silenced. Silence means that we have been forgotten and being forgotten is where injustice and uncertainty occurs. By using social media, pressing like on a post, or even sending a hate message, means that someone cares and is watching what you are doing. If there is no interaction, I am stuck in the land of indifference.
This is a place that I, and many others, now reside, captured and uncertain. In 2020, my plan was to graduate Cum Laude, dean's honor list, with three honors programs, three majors, and with research and job experience that stretched over six years. I would then go into my first year of graduate school, attempting a dual Juris Doctorate. I would be spending my time experimenting with new concepts, new experiences, and new relationships. My life would then be spent giving a microphone to survivors of domestic violence and sex crimes. However, now the plan is wiped clean, instead I sit still bound to graduate in 30 days with no home to stay, no place to work, and no future education to come back to. I would say I am overly qualified, but pandemic makes me lost in a series of names and masked faces.
Welcome to My Cage: The Pandemic and PTSD

When I read the campuswide email notifying students of the World Health Organization’s declaration of the coronavirus pandemic, I was sitting on my couch practicing a research presentation I was going to give a few hours later. For a few minutes, I sat there motionless, trying to digest the meaning of the words as though they were from a language other than my own, familiar sounds strung together in way that was wholly unintelligible to me. I tried but failed to make sense of how this could affect my life. After the initial shock had worn off, I mobilized quickly, snapping into an autopilot mode of being I knew all too well. I began making mental checklists, sharing the email with my friends and family, half of my brain wondering if I should make a trip to the grocery store to stockpile supplies and the other half wondering how I was supposed take final exams in the midst of so much uncertainty. The most chilling realization was knowing I had to wait powerlessly as the fate of the world unfolded, frozen with anxiety as I figured out my place in it all.
These feelings of powerlessness and isolation are familiar bedfellows for me. Early October of 2015, shortly after beginning my first year at UCI, I was diagnosed with Post-traumatic Stress Disorder. Despite having had years of psychological treatment for my condition, including Cognitive Behavior Therapy and Eye Movement Desensitization and Retraining, the flashbacks, paranoia, and nightmares still emerge unwarranted. People have referred to the pandemic as a collective trauma. For me, the pandemic has not only been a collective trauma, it has also been the reemergence of a personal trauma. The news of the pandemic and the implications it has for daily life triggered a reemergence of symptoms that were ultimately ignited by the overwhelming sense of helplessness that lies in waiting, as I suddenly find myself navigating yet another situation beyond my control. Food security, safety, and my sense of self have all been shaken by COVID-19.
The first few weeks after UCI transitioned into remote learning and the governor issued the stay-at-home order, I hardly got any sleep. My body was cycling through hypervigilance and derealization, and my sleep was interrupted by intrusive nightmares oscillating between flashbacks and frightening snippets from current events. Any coping methods I had developed through hard-won efforts over the past few years — leaving my apartment for a change of scenery, hanging out with friends, going to the gym — were suddenly made inaccessible to me due to the stay-at-home orders, closures of non-essential businesses, and many of my friends breaking their campus leases to move back to their family homes. So for me, learning to cope during COVID-19 quarantine means learning to function with my re-emerging PTSD symptoms and without my go-to tools. I must navigate my illness in a rapidly evolving world, one where some of my internalized fears, such as running out of food and living in an unsafe world, are made progressively more external by the minute and broadcasted on every news platform; fears that I could no longer escape, being confined in the tight constraints of my studio apartment’s walls. I cannot shake the devastating effects of sacrifice that I experience as all sense of control has been stripped away from me.
However, amidst my mental anguish, I have realized something important—experiencing these same PTSD symptoms during a global pandemic feels markedly different than it did years ago. Part of it might be the passage of time and the growth in my mindset, but there is something else that feels very different. Currently, there is widespread solidarity and support for all of us facing the chaos of COVID-19, whether they are on the frontlines of the fight against the illness or they are self-isolating due to new rules, restrictions, and risks. This was in stark contrast to what it was like to have a mental disorder. The unity we all experience as a result of COVID-19 is one I could not have predicted. I am not the only student heartbroken over a cancelled graduation, I am not the only student who is struggling to adapt to remote learning, and I am not the only person in this world who has to make sacrifices.
Between observations I’ve made on social media and conversations with my friends and classmates, this time we are all enduring great pain and stress as we attempt to adapt to life’s challenges. As a Peer Assistant for an Education class, I have heard from many students of their heartache over the remote learning model, how difficult it is to study in a non-academic environment, and how unmotivated they have become this quarter. This is definitely something I can relate to; as of late, it has been exceptionally difficult to find motivation and put forth the effort for even simple activities as a lack of energy compounds the issue and hinders basic needs. However, the willingness of people to open up about their distress during the pandemic is unlike the self-imposed social isolation of many people who experience mental illness regularly. Something this pandemic has taught me is that I want to live in a world where mental illness receives more support and isn’t so taboo and controversial. Why is it that we are able to talk about our pain, stress, and mental illness now, but aren’t able to talk about it outside of a global pandemic? People should be able to talk about these hardships and ask for help, much like during these circumstances.
It has been nearly three months since the coronavirus crisis was declared a pandemic. I still have many bad days that I endure where my symptoms can be overwhelming. But somehow, during my good days — and some days, merely good moments — I can appreciate the resilience I have acquired over the years and the common ground I share with others who live through similar circumstances. For veterans of trauma and mental illness, this isn’t the first time we are experiencing pain in an extreme and disastrous way. This is, however, the first time we are experiencing it with the rest of the world. This strange new feeling of solidarity as I read and hear about the experiences of other people provides some small comfort as I fight my way out of bed each day. As we fight to survive this pandemic, I hope to hold onto this feeling of togetherness and acceptance of pain, so that it will always be okay for people to share their struggles. We don’t know what the world will look like days, months, or years from now, but I hope that we can cultivate such a culture to make life much easier for people coping with mental illness.
A Somatic Pandemonium in Quarantine

I remember hearing that our brains create the color magenta all on their own.
When I was younger I used to run out of my third-grade class because my teacher was allergic to the mold and sometimes would vomit in the trash can. My dad used to tell me that I used to always have to have something in my hands, later translating itself into the form of a hair tie around my wrist.
Sometimes, I think about the girl who used to walk on her tippy toes. medial and lateral nerves never planted, never grounded. We were the same in this way. My ability to be firmly planted anywhere was also withered.
Was it from all the times I panicked? Or from the time I ran away and I blistered the soles of my feet 'til they were black from the summer pavement? Emetophobia.
I felt it in the shower, dressing itself from the crown of my head down to the soles of my feet, noting the feeling onto my white board in an attempt to solidify it’s permanence.
As I breathed in the chemical blue transpiring from the Expo marker, everything was more defined. I laid down and when I looked up at the starlet lamp I had finally felt centered. Still. No longer fleeting. The grooves in the lamps glass forming a spiral of what felt to me like an artificial landscape of transcendental sparks.
She’s back now, magenta, though I never knew she left or even ever was. Somehow still subconsciously always known. I had been searching for her in the tremors.
I can see her now in the daphnes, the golden rays from the sun reflecting off of the bark on the trees and the red light that glowed brighter, suddenly the town around me was warmer. A melting of hues and sharpened saturation that was apparent and reminded of the smell of oranges.
I threw up all of the carrots I ate just before. The trauma that my body kept as a memory of things that may or may not go wrong and the times that I couldn't keep my legs from running. Revelations bring memories bringing anxieties from fear and panic released from my body as if to say “NO LONGER!”
I close my eyes now and my mind's eye is, too, more vivid than ever before. My inner eyelids lit up with orange undertones no longer a solid black, neurons firing, fire. Not the kind that burns you but the kind that can light up a dull space. Like the wick of a tea-lit candle. Magenta doesn’t exist. It is perception. A construct made of light waves, blue and red.
Demolition. Reconstruction. I walk down the street into this new world wearing my new mask, somatic senses tingling and I think to myself “Houston, I think we’ve just hit equilibrium.”
How COVID-19 Changed My Senior Year

During the last two weeks of Winter quarter, I watched the emails pour in. Spring quarter would be online, facilities were closing, and everyone was recommended to return home to their families, if possible. I resolved to myself that I would not move back home; I wanted to stay in my apartment, near my boyfriend, near my friends, and in the one place I had my own space. However, as the COVID-19 pandemic worsened, things continued to change quickly. Soon I learned my roommate/best friend would be cancelling her lease and moving back up to Northern California. We had made plans for my final quarter at UCI, as I would be graduating in June while she had another year, but all of the sudden, that dream was gone. In one whirlwind of a day, we tried to cram in as much of our plans as we could before she left the next day for good. There are still so many things – like hiking, going to museums, and showing her around my hometown – we never got to cross off our list.
Then, my boyfriend decided he would also be moving home, three hours away. Most of my sorority sisters were moving home, too. I realized if I stayed at school, I would be completely alone. My mom had been encouraging me to move home anyway, but I was reluctant to return to a house I wasn’t completely comfortable in. As the pandemic became more serious, gentle encouragement quickly turned into demands. I had to cancel my lease and move home.
I moved back in with my parents at the end of Spring Break; I never got to say goodbye to most of my friends, many of whom I’ll likely never see again – as long as the virus doesn’t change things, I’m supposed to move to New York over the summer to begin a PhD program in Criminal Justice. Just like that, my time at UCI had come to a close. No lasts to savor; instead I had piles of things to regret. In place of a final quarter filled with memorable lasts, such as the senior banquet or my sorority’s senior preference night, I’m left with a laundry list of things I missed out on. I didn’t get to look around the campus one last time like I had planned; I never got to take my graduation pictures in front of the UC Irvine sign. Commencement had already been cancelled. The lights had turned off in the theatre before the movie was over. I never got to find out how the movie ended.
Transitioning to a remote learning system wasn’t too bad, but I found that some professors weren’t adjusting their courses to the difficulties many students were facing. It turned out to be difficult to stay motivated, especially for classes that are pre-recorded and don’t have any face-to-face interaction. It’s hard to make myself care; I’m in my last few weeks ever at UCI, but it feels like I’m already in summer. School isn’t real, my classes aren’t real. I still put in the effort, but I feel like I’m not getting much out of my classes.
The things I had been looking forward to this quarter are gone; there will be no Undergraduate Research Symposium, where I was supposed to present two projects. My amazing internship with the US Postal Inspection Service is over prematurely and I never got to properly say goodbye to anyone I met there. I won’t receive recognition for the various awards and honors I worked so hard to achieve.
And I’m one of the lucky ones! I feel guilty for feeling bad about my situation, when I know there are others who have it much, much worse. I am like that quintessential spoiled child, complaining while there are essential workers working tirelessly, people with health concerns constantly fearing for their safety, and people dying every day. Yet knowing that doesn't help me from feeling I was robbed of my senior experience, something I worked very hard to achieve. I know it’s not nearly as important as what many others are going through. But nevertheless, this is my situation. I was supposed to be enjoying this final quarter with my friends and preparing to move on, not be stuck at home, grappling with my mental health and hiding out in my room to get some alone time from a family I don’t always get along with. And while I know it’s more difficult out there for many others, it’s still difficult for me.
The thing that stresses me out most is the uncertainty. Uncertainty for the future – how long will this pandemic last? How many more people have to suffer before things go back to “normal” – whatever that is? How long until I can see my friends and family again? And what does this mean for my academic future? Who knows what will happen between now and then? All that’s left to do is wait and hope that everything will work out for the best.
Looking back over my last few months at UCI, I wish I knew at the time that I was experiencing my lasts; it feels like I took so much for granted. If there is one thing this has all made me realize, it’s that nothing is certain. Everything we expect, everything we take for granted – none of it is a given. Hold on to what you have while you have it, and take the time to appreciate the wonderful things in life, because you never know when it will be gone.
Physical Distancing

Thirty days have never felt so long. April has been the longest month of the year. I have been through more in these past three months than in the past three years. The COVID-19 outbreak has had a huge impact on both physical and social well-being of a lot of Americans, including me. Stress has been governing the lives of so many civilians, in particular students and workers. In addition to causing a lack of motivation in my life, quarantine has also brought a wave of anxiety.
My life changed the moment the Centers of Disease Control and Prevention and the government announced social distancing. My busy daily schedule, running from class to class and meeting to meeting, morphed into identical days, consisting of hour after hour behind a cold computer monitor. Human interaction and touch improve trust, reduce fear and increases physical well-being. Imagine the effects of removing the human touch and interaction from midst of society. Humans are profoundly social creatures. I cannot function without interacting and connecting with other people. Even daily acquaintances have an impact on me that is only noticeable once removed. As a result, the COVID-19 outbreak has had an extreme impact on me beyond direct symptoms and consequences of contracting the virus itself.
It was not until later that month, when out of sheer boredom I was scrolling through my call logs and I realized that I had called my grandmother more than ever. This made me realize that quarantine had created some positive impacts on my social interactions as well. This period of time has created an opportunity to check up on and connect with family and peers more often than we were able to. Even though we might be connecting solely through a screen, we are not missing out on being socially connected. Quarantine has taught me to value and prioritize social connection, and to recognize that we can find this type of connection not only through in-person gatherings, but also through deep heart to heart connections. Right now, my weekly Zoom meetings with my long-time friends are the most important events in my week. In fact, I have taken advantage of the opportunity to reconnect with many of my old friends and have actually had more meaningful conversations with them than before the isolation.
This situation is far from ideal. From my perspective, touch and in-person interaction is essential; however, we must overcome all difficulties that life throws at us with the best we are provided with. Therefore, perhaps we should take this time to re-align our motives by engaging in things that are of importance to us. I learned how to dig deep and find appreciation for all the small talks, gatherings, and face-to-face interactions. I have also realized that friendships are not only built on the foundation of physical presence but rather on meaningful conversations you get to have, even if they are through a cold computer monitor. My realization came from having more time on my hands and noticing the shift in conversations I was having with those around me. After all, maybe this isolation isn’t “social distancing”, but rather “physical distancing” until we meet again.
Follow us on social media
8 Lessons We Can Learn From the COVID-19 Pandemic
BY KATHY KATELLA May 14, 2021

Note: Information in this article was accurate at the time of original publication. Because information about COVID-19 changes rapidly, we encourage you to visit the websites of the Centers for Disease Control & Prevention (CDC), World Health Organization (WHO), and your state and local government for the latest information.
The COVID-19 pandemic changed life as we know it—and it may have changed us individually as well, from our morning routines to our life goals and priorities. Many say the world has changed forever. But this coming year, if the vaccines drive down infections and variants are kept at bay, life could return to some form of normal. At that point, what will we glean from the past year? Are there silver linings or lessons learned?
“Humanity's memory is short, and what is not ever-present fades quickly,” says Manisha Juthani, MD , a Yale Medicine infectious diseases specialist. The bubonic plague, for example, ravaged Europe in the Middle Ages—resurfacing again and again—but once it was under control, people started to forget about it, she says. “So, I would say one major lesson from a public health or infectious disease perspective is that it’s important to remember and recognize our history. This is a period we must remember.”
We asked our Yale Medicine experts to weigh in on what they think are lessons worth remembering, including those that might help us survive a future virus or nurture a resilience that could help with life in general.
Lesson 1: Masks are useful tools
What happened: The Centers for Disease Control and Prevention (CDC) relaxed its masking guidance for those who have been fully vaccinated. But when the pandemic began, it necessitated a global effort to ensure that everyone practiced behaviors to keep themselves healthy and safe—and keep others healthy as well. This included the widespread wearing of masks indoors and outside.
What we’ve learned: Not everyone practiced preventive measures such as mask wearing, maintaining a 6-foot distance, and washing hands frequently. But, Dr. Juthani says, “I do think many people have learned a whole lot about respiratory pathogens and viruses, and how they spread from one person to another, and that sort of old-school common sense—you know, if you don’t feel well—whether it’s COVID-19 or not—you don’t go to the party. You stay home.”
Masks are a case in point. They are a key COVID-19 prevention strategy because they provide a barrier that can keep respiratory droplets from spreading. Mask-wearing became more common across East Asia after the 2003 SARS outbreak in that part of the world. “There are many East Asian cultures where the practice is still that if you have a cold or a runny nose, you put on a mask,” Dr. Juthani says.
She hopes attitudes in the U.S. will shift in that direction after COVID-19. “I have heard from a number of people who are amazed that we've had no flu this year—and they know masks are one of the reasons,” she says. “They’ve told me, ‘When the winter comes around, if I'm going out to the grocery store, I may just put on a mask.’”
Lesson 2: Telehealth might become the new normal
What happened: Doctors and patients who have used telehealth (technology that allows them to conduct medical care remotely), found it can work well for certain appointments, ranging from cardiology check-ups to therapy for a mental health condition. Many patients who needed a medical test have also discovered it may be possible to substitute a home version.
What we’ve learned: While there are still problems for which you need to see a doctor in person, the pandemic introduced a new urgency to what had been a gradual switchover to platforms like Zoom for remote patient visits.
More doctors also encouraged patients to track their blood pressure at home , and to use at-home equipment for such purposes as diagnosing sleep apnea and even testing for colon cancer . Doctors also can fine-tune cochlear implants remotely .
“It happened very quickly,” says Sharon Stoll, DO, a neurologist. One group that has benefitted is patients who live far away, sometimes in other parts of the country—or even the world, she says. “I always like to see my patients at least twice a year. Now, we can see each other in person once a year, and if issues come up, we can schedule a telehealth visit in-between,” Dr. Stoll says. “This way I may hear about an issue before it becomes a problem, because my patients have easier access to me, and I have easier access to them.”
Meanwhile, insurers are becoming more likely to cover telehealth, Dr. Stoll adds. “That is a silver lining that will hopefully continue.”
Lesson 3: Vaccines are powerful tools
What happened: Given the recent positive results from vaccine trials, once again vaccines are proving to be powerful for preventing disease.
What we’ve learned: Vaccines really are worth getting, says Dr. Stoll, who had COVID-19 and experienced lingering symptoms, including chronic headaches . “I have lots of conversations—and sometimes arguments—with people about vaccines,” she says. Some don’t like the idea of side effects. “I had vaccine side effects and I’ve had COVID-19 side effects, and I say nothing compares to the actual illness. Unfortunately, I speak from experience.”
Dr. Juthani hopes the COVID-19 vaccine spotlight will motivate people to keep up with all of their vaccines, including childhood and adult vaccines for such diseases as measles , chicken pox, shingles , and other viruses. She says people have told her they got the flu vaccine this year after skipping it in previous years. (The CDC has reported distributing an exceptionally high number of doses this past season.)
But, she cautions that a vaccine is not a magic bullet—and points out that scientists can’t always produce one that works. “As advanced as science is, there have been multiple failed efforts to develop a vaccine against the HIV virus,” she says. “This time, we were lucky that we were able build on the strengths that we've learned from many other vaccine development strategies to develop multiple vaccines for COVID-19 .”
Lesson 4: Everyone is not treated equally, especially in a pandemic
What happened: COVID-19 magnified disparities that have long been an issue for a variety of people.
What we’ve learned: Racial and ethnic minority groups especially have had disproportionately higher rates of hospitalization for COVID-19 than non-Hispanic white people in every age group, and many other groups faced higher levels of risk or stress. These groups ranged from working mothers who also have primary responsibility for children, to people who have essential jobs, to those who live in rural areas where there is less access to health care.
“One thing that has been recognized is that when people were told to work from home, you needed to have a job that you could do in your house on a computer,” says Dr. Juthani. “Many people who were well off were able do that, but they still needed to have food, which requires grocery store workers and truck drivers. Nursing home residents still needed certified nursing assistants coming to work every day to care for them and to bathe them.”
As far as racial inequities, Dr. Juthani cites President Biden’s appointment of Yale Medicine’s Marcella Nunez-Smith, MD, MHS , as inaugural chair of a federal COVID-19 Health Equity Task Force. “Hopefully the new focus is a first step,” Dr. Juthani says.
Lesson 5: We need to take mental health seriously
What happened: There was a rise in reported mental health problems that have been described as “a second pandemic,” highlighting mental health as an issue that needs to be addressed.
What we’ve learned: Arman Fesharaki-Zadeh, MD, PhD , a behavioral neurologist and neuropsychiatrist, believes the number of mental health disorders that were on the rise before the pandemic is surging as people grapple with such matters as juggling work and childcare, job loss, isolation, and losing a loved one to COVID-19.
The CDC reports that the percentage of adults who reported symptoms of anxiety of depression in the past 7 days increased from 36.4 to 41.5 % from August 2020 to February 2021. Other reports show that having COVID-19 may contribute, too, with its lingering or long COVID symptoms, which can include “foggy mind,” anxiety , depression, and post-traumatic stress disorder .
“We’re seeing these problems in our clinical setting very, very often,” Dr. Fesharaki-Zadeh says. “By virtue of necessity, we can no longer ignore this. We're seeing these folks, and we have to take them seriously.”
Lesson 6: We have the capacity for resilience
What happened: While everyone’s situation is different (and some people have experienced tremendous difficulties), many have seen that it’s possible to be resilient in a crisis.
What we’ve learned: People have practiced self-care in a multitude of ways during the pandemic as they were forced to adjust to new work schedules, change their gym routines, and cut back on socializing. Many started seeking out new strategies to counter the stress.
“I absolutely believe in the concept of resilience, because we have this effective reservoir inherent in all of us—be it the product of evolution, or our ancestors going through catastrophes, including wars, famines, and plagues,” Dr. Fesharaki-Zadeh says. “I think inherently, we have the means to deal with crisis. The fact that you and I are speaking right now is the result of our ancestors surviving hardship. I think resilience is part of our psyche. It's part of our DNA, essentially.”
Dr. Fesharaki-Zadeh believes that even small changes are highly effective tools for creating resilience. The changes he suggests may sound like the same old advice: exercise more, eat healthy food, cut back on alcohol, start a meditation practice, keep up with friends and family. “But this is evidence-based advice—there has been research behind every one of these measures,” he says.
But we have to also be practical, he notes. “If you feel overwhelmed by doing too many things, you can set a modest goal with one new habit—it could be getting organized around your sleep. Once you’ve succeeded, move on to another one. Then you’re building momentum.”
Lesson 7: Community is essential—and technology is too
What happened: People who were part of a community during the pandemic realized the importance of human connection, and those who didn’t have that kind of support realized they need it.
What we’ve learned: Many of us have become aware of how much we need other people—many have managed to maintain their social connections, even if they had to use technology to keep in touch, Dr. Juthani says. “There's no doubt that it's not enough, but even that type of community has helped people.”
Even people who aren’t necessarily friends or family are important. Dr. Juthani recalled how she encouraged her mail carrier to sign up for the vaccine, soon learning that the woman’s mother and husband hadn’t gotten it either. “They are all vaccinated now,” Dr. Juthani says. “So, even by word of mouth, community is a way to make things happen.”
It’s important to note that some people are naturally introverted and may have enjoyed having more solitude when they were forced to stay at home—and they should feel comfortable with that, Dr. Fesharaki-Zadeh says. “I think one has to keep temperamental tendencies like this in mind.”
But loneliness has been found to suppress the immune system and be a precursor to some diseases, he adds. “Even for introverted folks, the smallest circle is preferable to no circle at all,” he says.
Lesson 8: Sometimes you need a dose of humility
What happened: Scientists and nonscientists alike learned that a virus can be more powerful than they are. This was evident in the way knowledge about the virus changed over time in the past year as scientific investigation of it evolved.
What we’ve learned: “As infectious disease doctors, we were resident experts at the beginning of the pandemic because we understand pathogens in general, and based on what we’ve seen in the past, we might say there are certain things that are likely to be true,” Dr. Juthani says. “But we’ve seen that we have to take these pathogens seriously. We know that COVID-19 is not the flu. All these strokes and clots, and the loss of smell and taste that have gone on for months are things that we could have never known or predicted. So, you have to have respect for the unknown and respect science, but also try to give scientists the benefit of the doubt,” she says.
“We have been doing the best we can with the knowledge we have, in the time that we have it,” Dr. Juthani says. “I think most of us have had to have the humility to sometimes say, ‘I don't know. We're learning as we go.’"
Information provided in Yale Medicine articles is for general informational purposes only. No content in the articles should ever be used as a substitute for medical advice from your doctor or other qualified clinician. Always seek the individual advice of your health care provider with any questions you have regarding a medical condition.
More news from Yale Medicine

The pandemic has had devastating impacts on learning. What will it take to help students catch up?
Subscribe to the brown center on education policy newsletter, megan kuhfeld , megan kuhfeld senior research scientist - nwea jim soland , jim soland assistant professor, school of education and human development - university of virginia, affiliated research fellow - nwea karyn lewis , and karyn lewis director, center for school and student progress - nwea emily morton emily morton research scientist - nwea.
March 3, 2022
As we reach the two-year mark of the initial wave of pandemic-induced school shutdowns, academic normalcy remains out of reach for many students, educators, and parents. In addition to surging COVID-19 cases at the end of 2021, schools have faced severe staff shortages , high rates of absenteeism and quarantines , and rolling school closures . Furthermore, students and educators continue to struggle with mental health challenges , higher rates of violence and misbehavior , and concerns about lost instructional time .
As we outline in our new research study released in January, the cumulative impact of the COVID-19 pandemic on students’ academic achievement has been large. We tracked changes in math and reading test scores across the first two years of the pandemic using data from 5.4 million U.S. students in grades 3-8. We focused on test scores from immediately before the pandemic (fall 2019), following the initial onset (fall 2020), and more than one year into pandemic disruptions (fall 2021).
Average fall 2021 math test scores in grades 3-8 were 0.20-0.27 standard deviations (SDs) lower relative to same-grade peers in fall 2019, while reading test scores were 0.09-0.18 SDs lower. This is a sizable drop. For context, the math drops are significantly larger than estimated impacts from other large-scale school disruptions, such as after Hurricane Katrina—math scores dropped 0.17 SDs in one year for New Orleans evacuees .
Even more concerning, test-score gaps between students in low-poverty and high-poverty elementary schools grew by approximately 20% in math (corresponding to 0.20 SDs) and 15% in reading (0.13 SDs), primarily during the 2020-21 school year. Further, achievement tended to drop more between fall 2020 and 2021 than between fall 2019 and 2020 (both overall and differentially by school poverty), indicating that disruptions to learning have continued to negatively impact students well past the initial hits following the spring 2020 school closures.
These numbers are alarming and potentially demoralizing, especially given the heroic efforts of students to learn and educators to teach in incredibly trying times. From our perspective, these test-score drops in no way indicate that these students represent a “ lost generation ” or that we should give up hope. Most of us have never lived through a pandemic, and there is so much we don’t know about students’ capacity for resiliency in these circumstances and what a timeline for recovery will look like. Nor are we suggesting that teachers are somehow at fault given the achievement drops that occurred between 2020 and 2021; rather, educators had difficult jobs before the pandemic, and now are contending with huge new challenges, many outside their control.
Clearly, however, there’s work to do. School districts and states are currently making important decisions about which interventions and strategies to implement to mitigate the learning declines during the last two years. Elementary and Secondary School Emergency Relief (ESSER) investments from the American Rescue Plan provided nearly $200 billion to public schools to spend on COVID-19-related needs. Of that sum, $22 billion is dedicated specifically to addressing learning loss using “evidence-based interventions” focused on the “ disproportionate impact of COVID-19 on underrepresented student subgroups. ” Reviews of district and state spending plans (see Future Ed , EduRecoveryHub , and RAND’s American School District Panel for more details) indicate that districts are spending their ESSER dollars designated for academic recovery on a wide variety of strategies, with summer learning, tutoring, after-school programs, and extended school-day and school-year initiatives rising to the top.
Comparing the negative impacts from learning disruptions to the positive impacts from interventions
To help contextualize the magnitude of the impacts of COVID-19, we situate test-score drops during the pandemic relative to the test-score gains associated with common interventions being employed by districts as part of pandemic recovery efforts. If we assume that such interventions will continue to be as successful in a COVID-19 school environment, can we expect that these strategies will be effective enough to help students catch up? To answer this question, we draw from recent reviews of research on high-dosage tutoring , summer learning programs , reductions in class size , and extending the school day (specifically for literacy instruction) . We report effect sizes for each intervention specific to a grade span and subject wherever possible (e.g., tutoring has been found to have larger effects in elementary math than in reading).
Figure 1 shows the standardized drops in math test scores between students testing in fall 2019 and fall 2021 (separately by elementary and middle school grades) relative to the average effect size of various educational interventions. The average effect size for math tutoring matches or exceeds the average COVID-19 score drop in math. Research on tutoring indicates that it often works best in younger grades, and when provided by a teacher rather than, say, a parent. Further, some of the tutoring programs that produce the biggest effects can be quite intensive (and likely expensive), including having full-time tutors supporting all students (not just those needing remediation) in one-on-one settings during the school day. Meanwhile, the average effect of reducing class size is negative but not significant, with high variability in the impact across different studies. Summer programs in math have been found to be effective (average effect size of .10 SDs), though these programs in isolation likely would not eliminate the COVID-19 test-score drops.
Figure 1: Math COVID-19 test-score drops compared to the effect sizes of various educational interventions

Source: COVID-19 score drops are pulled from Kuhfeld et al. (2022) Table 5; reduction-in-class-size results are from pg. 10 of Figles et al. (2018) Table 2; summer program results are pulled from Lynch et al (2021) Table 2; and tutoring estimates are pulled from Nictow et al (2020) Table 3B. Ninety-five percent confidence intervals are shown with vertical lines on each bar.
Notes: Kuhfeld et al. and Nictow et al. reported effect sizes separately by grade span; Figles et al. and Lynch et al. report an overall effect size across elementary and middle grades. We were unable to find a rigorous study that reported effect sizes for extending the school day/year on math performance. Nictow et al. and Kraft & Falken (2021) also note large variations in tutoring effects depending on the type of tutor, with larger effects for teacher and paraprofessional tutoring programs than for nonprofessional and parent tutoring. Class-size reductions included in the Figles meta-analysis ranged from a minimum of one to minimum of eight students per class.
Figure 2 displays a similar comparison using effect sizes from reading interventions. The average effect of tutoring programs on reading achievement is larger than the effects found for the other interventions, though summer reading programs and class size reduction both produced average effect sizes in the ballpark of the COVID-19 reading score drops.
Figure 2: Reading COVID-19 test-score drops compared to the effect sizes of various educational interventions

Source: COVID-19 score drops are pulled from Kuhfeld et al. (2022) Table 5; extended-school-day results are from Figlio et al. (2018) Table 2; reduction-in-class-size results are from pg. 10 of Figles et al. (2018) ; summer program results are pulled from Kim & Quinn (2013) Table 3; and tutoring estimates are pulled from Nictow et al (2020) Table 3B. Ninety-five percent confidence intervals are shown with vertical lines on each bar.
Notes: While Kuhfeld et al. and Nictow et al. reported effect sizes separately by grade span, Figlio et al. and Kim & Quinn report an overall effect size across elementary and middle grades. Class-size reductions included in the Figles meta-analysis ranged from a minimum of one to minimum of eight students per class.
There are some limitations of drawing on research conducted prior to the pandemic to understand our ability to address the COVID-19 test-score drops. First, these studies were conducted under conditions that are very different from what schools currently face, and it is an open question whether the effectiveness of these interventions during the pandemic will be as consistent as they were before the pandemic. Second, we have little evidence and guidance about the efficacy of these interventions at the unprecedented scale that they are now being considered. For example, many school districts are expanding summer learning programs, but school districts have struggled to find staff interested in teaching summer school to meet the increased demand. Finally, given the widening test-score gaps between low- and high-poverty schools, it’s uncertain whether these interventions can actually combat the range of new challenges educators are facing in order to narrow these gaps. That is, students could catch up overall, yet the pandemic might still have lasting, negative effects on educational equality in this country.
Given that the current initiatives are unlikely to be implemented consistently across (and sometimes within) districts, timely feedback on the effects of initiatives and any needed adjustments will be crucial to districts’ success. The Road to COVID Recovery project and the National Student Support Accelerator are two such large-scale evaluation studies that aim to produce this type of evidence while providing resources for districts to track and evaluate their own programming. Additionally, a growing number of resources have been produced with recommendations on how to best implement recovery programs, including scaling up tutoring , summer learning programs , and expanded learning time .
Ultimately, there is much work to be done, and the challenges for students, educators, and parents are considerable. But this may be a moment when decades of educational reform, intervention, and research pay off. Relying on what we have learned could show the way forward.
Related Content
Megan Kuhfeld, Jim Soland, Beth Tarasawa, Angela Johnson, Erik Ruzek, Karyn Lewis
December 3, 2020
Lindsay Dworkin, Karyn Lewis
October 13, 2021
Early Childhood Education Education Access & Equity Education Policy K-12 Education
Governance Studies
U.S. States and Territories
Brown Center on Education Policy
Magdalena Rodríguez Romero
September 10, 2024
Tom Swiderski, Sarah Crittenden Fuller, Kevin C. Bastian
September 9, 2024
Julien Lafortune, Barbara Biasi, David Schönholzer
September 6, 2024
- Fact sheets
- Facts in pictures
- Publications
- Questions and answers
- Tools and toolkits
- Endometriosis
- Excessive heat
- Mental disorders
- Polycystic ovary syndrome
- All countries
- Eastern Mediterranean
- South-East Asia
- Western Pacific
- Data by country
- Country presence
- Country strengthening
- Country cooperation strategies
- News releases
- Feature stories
- Press conferences
- Commentaries
- Photo library
- Afghanistan
- Cholera
- Coronavirus disease (COVID-19)
- Greater Horn of Africa
- Israel and occupied Palestinian territory
- Disease Outbreak News
- Situation reports
- Weekly Epidemiological Record
- Surveillance
- Health emergency appeal
- International Health Regulations
- Independent Oversight and Advisory Committee
- Classifications
- Data collections
- Global Health Observatory
- Global Health Estimates
- Mortality Database
- Sustainable Development Goals
- Health Inequality Monitor
- Global Progress
- World Health Statistics
- Partnerships
- Committees and advisory groups
- Collaborating centres
- Technical teams
- Organizational structure
- Initiatives
- General Programme of Work
- WHO Academy
- Investment in WHO
- WHO Foundation
- External audit
- Financial statements
- Internal audit and investigations
- Programme Budget
- Results reports
- Governing bodies
- World Health Assembly
- Executive Board
- Member States Portal
Impact of COVID-19 on people's livelihoods, their health and our food systems
Joint statement by ilo, fao, ifad and who.
The COVID-19 pandemic has led to a dramatic loss of human life worldwide and presents an unprecedented challenge to public health, food systems and the world of work. The economic and social disruption caused by the pandemic is devastating: tens of millions of people are at risk of falling into extreme poverty, while the number of undernourished people, currently estimated at nearly 690 million, could increase by up to 132 million by the end of the year.
Millions of enterprises face an existential threat. Nearly half of the world’s 3.3 billion global workforce are at risk of losing their livelihoods. Informal economy workers are particularly vulnerable because the majority lack social protection and access to quality health care and have lost access to productive assets. Without the means to earn an income during lockdowns, many are unable to feed themselves and their families. For most, no income means no food, or, at best, less food and less nutritious food.
The pandemic has been affecting the entire food system and has laid bare its fragility. Border closures, trade restrictions and confinement measures have been preventing farmers from accessing markets, including for buying inputs and selling their produce, and agricultural workers from harvesting crops, thus disrupting domestic and international food supply chains and reducing access to healthy, safe and diverse diets. The pandemic has decimated jobs and placed millions of livelihoods at risk. As breadwinners lose jobs, fall ill and die, the food security and nutrition of millions of women and men are under threat, with those in low-income countries, particularly the most marginalized populations, which include small-scale farmers and indigenous peoples, being hardest hit.
Millions of agricultural workers – waged and self-employed – while feeding the world, regularly face high levels of working poverty, malnutrition and poor health, and suffer from a lack of safety and labour protection as well as other types of abuse. With low and irregular incomes and a lack of social support, many of them are spurred to continue working, often in unsafe conditions, thus exposing themselves and their families to additional risks. Further, when experiencing income losses, they may resort to negative coping strategies, such as distress sale of assets, predatory loans or child labour. Migrant agricultural workers are particularly vulnerable, because they face risks in their transport, working and living conditions and struggle to access support measures put in place by governments. Guaranteeing the safety and health of all agri-food workers – from primary producers to those involved in food processing, transport and retail, including street food vendors – as well as better incomes and protection, will be critical to saving lives and protecting public health, people’s livelihoods and food security.
In the COVID-19 crisis food security, public health, and employment and labour issues, in particular workers’ health and safety, converge. Adhering to workplace safety and health practices and ensuring access to decent work and the protection of labour rights in all industries will be crucial in addressing the human dimension of the crisis. Immediate and purposeful action to save lives and livelihoods should include extending social protection towards universal health coverage and income support for those most affected. These include workers in the informal economy and in poorly protected and low-paid jobs, including youth, older workers, and migrants. Particular attention must be paid to the situation of women, who are over-represented in low-paid jobs and care roles. Different forms of support are key, including cash transfers, child allowances and healthy school meals, shelter and food relief initiatives, support for employment retention and recovery, and financial relief for businesses, including micro, small and medium-sized enterprises. In designing and implementing such measures it is essential that governments work closely with employers and workers.
Countries dealing with existing humanitarian crises or emergencies are particularly exposed to the effects of COVID-19. Responding swiftly to the pandemic, while ensuring that humanitarian and recovery assistance reaches those most in need, is critical.
Now is the time for global solidarity and support, especially with the most vulnerable in our societies, particularly in the emerging and developing world. Only together can we overcome the intertwined health and social and economic impacts of the pandemic and prevent its escalation into a protracted humanitarian and food security catastrophe, with the potential loss of already achieved development gains.
We must recognize this opportunity to build back better, as noted in the Policy Brief issued by the United Nations Secretary-General. We are committed to pooling our expertise and experience to support countries in their crisis response measures and efforts to achieve the Sustainable Development Goals. We need to develop long-term sustainable strategies to address the challenges facing the health and agri-food sectors. Priority should be given to addressing underlying food security and malnutrition challenges, tackling rural poverty, in particular through more and better jobs in the rural economy, extending social protection to all, facilitating safe migration pathways and promoting the formalization of the informal economy.
We must rethink the future of our environment and tackle climate change and environmental degradation with ambition and urgency. Only then can we protect the health, livelihoods, food security and nutrition of all people, and ensure that our ‘new normal’ is a better one.
Media Contacts
Kimberly Chriscaden
Communications Officer World Health Organization
Nutrition and Food Safety (NFS) and COVID-19
An examination of COVID-19’s impact on student learning: a self-determination theory perspective
- September 2024
- This person is not on ResearchGate, or hasn't claimed this research yet.

- University of Kentucky

Discover the world's research
- 25+ million members
- 160+ million publication pages
- 2.3+ billion citations
No full-text available
To read the full-text of this research, you can request a copy directly from the authors.

- Saeed Pahlevansharif
- Thomas Babalis
- Konstantina Tsoli
- PSYCHIAT RES

- Kaylene Godfrey

- BEHAV CHANGE

- Charlotte Branchu
- Erwin Flaureau

- Hsin-Te Yeh
- Ying-Chia Hsu

- Matthew LaGrone
- Shenoa Ragavaloo

- Dominic Conroy

- Angela Paladino
- Robert J. Summers

- BMC PSYCHIATRY

- Lars Johan Danbolt

- Martin V. Bonsangue
- Jennifer E. Clinkenbeard

- J AM COLL HEALTH

- Josep Petchamé

- William Talley
- Bridget Irioogbe

- EDUC PSYCHOL REV

- J MED INTERNET RES

- INT J SOC PSYCHIATR

- John P. Bean
- Russell K. Bradley
- David G. Taylor
- Michael Frechette
- Sheryl-Ann K. Stephen
- Marleen McCormick-Pritchard
- James W. Peltier

- Sherry Davis Molock

- Chad E. Kee
- Holly Hapke
- Tereza Dean
- J PUBLIC ECON

- Jacob French

- Basit Zafar
- Jianzhong Zheng

- LEARN INSTR

- James C. Lester

- Petra Brock

- Dean B. McFarlin
- Paul D. Sweeney
- Peter M. Bentler
- Decis Sci J Innovat Educ

- ANNU REV PSYCHOL
- Nathan P. Podsakoff
- Recruit researchers
- Join for free
- Login Email Tip: Most researchers use their institutional email address as their ResearchGate login Password Forgot password? Keep me logged in Log in or Continue with Google Welcome back! Please log in. Email · Hint Tip: Most researchers use their institutional email address as their ResearchGate login Password Forgot password? Keep me logged in Log in or Continue with Google No account? Sign up
IMAGES
VIDEO
COMMENTS
This year, the Common App is including a special 250-word section allowing students to describe the impacts of COVID-19 on their lives. Here's the official word from the Common App website: . We want to provide colleges with the information they need, with the goal of having students answer COVID-19 questions only once while using the rest of the application as they would have before to ...
Writing About COVID-19 in College Essays. Experts say students should be honest and not limit themselves to merely their experiences with the pandemic. The global impact of COVID-19, the disease ...
Please find below a sample of a short essay on Covid-19 for school students: Also Read: Essay on Women's Day in 200 and 500 words. FAQs. How to write an essay on COVID-19? to write an essay on COVID-19, understand your word limit and make sure to cover all the stages and symptoms of this disease. You need to highlight all the challenges and ...
Introduction. The global outbreak of COVID-19 has certainly taken an overwhelming toll on everyone. People have lost their jobs, their homes, and even their lives. There is no getting past the fact that the overall impact on the world has been negative, but it is important to realize that positive aspects of the pandemic have been overshadowed ...
variation in the e ects of COVID-19 across students. In terms of labor market expectations, on average, students foresee a 13 percentage points decrease in. the probability of. on, a reduction of 2 percent in their reservation wages, a. d a2.3 percent decrease in their expected earn. ID-19 demonstrate that stude.
Students working on college admission essays often struggle to figure out how to write about their experiences during the COVID-19 pandemic. For students applying to college using the CommonApp, there are several different places where students and counselors can address the pandemic's impact. The different sections have differing goals.
In almost all grades, the majority of students made some learning gains in both reading and math since the COVID-19 pandemic started, though gains were smaller in math in 2020 relative to the ...
The global impact of COVID-19, the disease caused by the novel coronavirus, means colleges and prospective students alike are in for an admissions cycle like no other. Major college admissions ...
This year the Common App, the nation's most-used application, added a question inviting students to write about the impact of Covid-19 on their lives and educations.
%PDF-1.5 %¿÷¢þ 4 0 obj /Linearized 1 /L 38547 /H [ 687 136 ] /O 8 /E 35516 /N 2 /T 38261 >> endobj 5 0 obj /Type /XRef /Length 51 /Filter /FlateDecode ...
In these short essays below, teacher Claire Marie Grogan's 11th grade students at Oceanside High School on Long Island, N.Y., describe their pandemic experiences. ... My mom had COVID-19 for ten ...
For Black students, the number spikes to 25 percent. "There are many reasons to believe the Covid-19 impacts might be larger for children in poverty and children of color," Kuhfeld wrote in the study. Their families suffer higher rates of infection, and the economic burden disproportionately falls on Black and Hispanic parents, who are less ...
The COVID-19 pandemic has had a profound impact on individuals, societies, and economies worldwide. Its multifaceted nature presents a wealth of topics suitable for academic exploration. This essay provides guidance on developing engaging and insightful essay topics related to COVID-19, offering a comprehensive range of perspectives to choose from.
The students enjoyed seeing how this idea can drive both domestic and international health policies." A sampling of the published student essays are below: Alexander Giummo '22 and Mike Dunderdale's '23 op-ed titled "A National Testing Proposal: Let's Fight Back Against COVID-19" was published in the Journal Inquirer in Manchester ...
A Catalogue of 300 Best Persuasive Essay Topics for Students; Persuasive Essay Outline - A Complete Guide; 30+ Persuasive Essay Examples To Get You Started; ... Impact of COVID-19 Essay. Covid19, also known as Coronavirus, is an infectious disease that has had a major impact on the world. Since its emergence in late 2019, COVID-19 has infected ...
Our findings on academic outcomes indicate that COVID-19 has led to a large number of students delaying graduation (13%), withdrawing from classes (11%), and intending to change majors (12%). Moreover, approximately 50% of our sample separately reported a decrease in study hours and in their academic performance.
Background/aim In the beginning of 2020, the novel Coronavirus disease (COVID-19) caused by the SARS-CoV-2 virus, became a public health emergency in the U.S. and rapidly escalated into a global pandemic. Because the SARS-CoV-2 virus is highly contagious, physical distancing was enforced and indoor public spaces, including schools and educational institutions, were abruptly closed and ...
The COVID-19 outbreak has had a huge impact on both physical and social well-being of a lot of Americans, including me. Stress has been governing the lives of so many civilians, in particular students and workers. In addition to causing a lack of motivation in my life, quarantine has also brought a wave of anxiety.
The CDC reports that the percentage of adults who reported symptoms of anxiety of depression in the past 7 days increased from 36.4 to 41.5 % from August 2020 to February 2021. Other reports show that having COVID-19 may contribute, too, with its lingering or long COVID symptoms, which can include "foggy mind," anxiety, depression, and post ...
A student wearing a protective mask, attends class on the first day of school, amid the coronavirus disease (COVID-19) pandemic, at St. Lawrence Catholic School in North Miami Beach, Florida, U.S ...
My first two thoughts were mixtures of empathetic concern and selfish relief— "I'm glad I did my study abroad in the fall" and "It must be really tough to be a college senior this year ...
Reading time: 3 min (864 words) The COVID-19 pandemic has led to a dramatic loss of human life worldwide and presents an unprecedented challenge to public health, food systems and the world of work. The economic and social disruption caused by the pandemic is devastating: tens of millions of people are at risk of falling into extreme poverty ...
The purpose of the study is to investigate how African American students cope with the severe impact of COVID‐19 on their emotional well‐being leveraging the benefits of self‐care coping ...